Cold and flu season is here. And if you have children, that’s not good news. Children and adolescents are particularly susceptible to respiratory infections (colds, sore throat, sinusitis, pneumonia, and bronchitis). That’s because:
Their immune systems are immature.
Their diet and sleep patterns are far from optimal.
Increasing environmental pollution makes the problem worse.
And that’s a problem. The WHO says:
Respiratory diseases are the leading cause of childhood deaths globally.
RSV alone results in 3.6 million hospitalizations and 100,000 deaths each year.
The death rates are not as high in the US, but every day your child is sick at home:
They are not in school leaning.
One parent has to stay home from their job to take care of them.
If you want to protect your child from respiratory infections and do it naturally, you need to strengthen their immune system. And that requires a holistic approach which I have described in a previous issue of “Health Tips From The Professor”.
But ever since Dr. Linus Pauling published “Vitamin C and the Common Cold” in 1970, there has been a lot of discussion about the role of vitamin C in preventing respiratory infections. I don’t need to tell you this has been a controversial topic.
Several recent studies have confirmed the role of vitamin C in preventing and shortening respiratory infections in adults, and this did not require the mega-dose levels recommended by Dr. Pauling.
However, high-quality studies on the role of preventing respiratory infections in children and adolescents are lacking. The study (C Li et al, Frontiers in Nutrition, 12:1601218, 2025) I will describe today was designed to fill this gap.
How Was This Study Done?
The authors of this study used data from the 2017-2018 National Health and Nutrition Examination Survey (NHANES) in the United States. The NHANES study included 8,704 people, of which 1,344 were children or adolescents aged 6-19 years old.
At the time of enrollment:
Serum levels of vitamin C were determined by laboratory analysis.
The incidence of recent (within 30 days) respiratory infections was determined from a self-reported health questionnaire. In this study the most frequent respiratory infection was the common cold. But the term respiratory infections also included sore throats, sinusitis, pneumonia, and bronchitis.
Of the 1,344 participants, 238 (17.7%) reported a respiratory infection within the past 30 days.
The participants were divided into quartiles based on serum levels of vitamin C, and the highest versus lowest quartiles were compared for the risk of developing respiratory infections.
Finally, the data were statistically corrected for confounding variables like sex, age, race, obesity, asthma, and tobacco smoke exposure.
Can Vitamin C Reduce Colds in Children?
The results were clear cut:
There was a significant negative association between serum levels of vitamin C and the risk of respiratory infections (In plain English that means as serum levels of vitamin C increased, the risk of respiratory infections decreased).
For every 10 unit increase in serum vitamin C levels, the risk of respiratory disease decreased by 7%.
Children and adolescents in the top quartile of serum vitamin C were 50% less likely to develop a respiratory infection than those in the bottom quartile.
Based on previous studies, the authors said the most likely mechanisms for the effect of vitamin C on the risk of developing a respiratory disease are:
Vitamin C exerts antioxidant protection against free radicals generated by immune cells, which protects the integrity of cells lining the respiratory track.
2) Vitamin C strengths the ability of neutrophils to clear pathogens (bacteria and viruses) from the blood.
3) Vitamin C inhibits pro-inflammatory cytokines, thereby reducing inflammatory responses that can worsen and prolong respiratory infections.
The authors concluded,
“This study demonstrates a negative association between serum vitamin C and respiratory infection risk in a nationally representative sample of children and adolescents.
These findings highlight the protective role of vitamin C against respiratory infections and underscore the importance of maintaining optimal vitamin C levels.
Our findings suggest that vitamin C supplementation may be potentially used for the prevention and treatment of respiratory infections among children and adolescents.”
What Does This Study Mean For You?
This study suggests that vitamin C supplementation may help protect our children and grandchildren from respiratory infections. However, we need to acknowledge the strengths and limitations of the study.
On the positive side, this study is fully consistent with previous studies showing that vitamin C supplementation reduces the risk of getting respiratory infections in adults – and reduces the duration and severity of respiratory infections when they do occur.
On the negative side, this is a single study. It highlights the need for more studies of the effect of vitamin C on respiratory infections in children.
You also may be thinking, “This study talks in terms of serum levels of vitamin C. It doesn’t tell me how much vitamin C my children and grandchildren should be getting.”
There is a good reason this study was based on serum levels of vitamin C. It’s the most accurate measure of vitamin C status.
Intake of vitamin C based on dietary questionnaires is often inaccurate.
There is not a linear relationship between dietary vitamin C and serum levels of vitamin C.
Serum levels of vitamin C can be influenced by obesity and other metabolic and disease states.
So, I have done a little research to give you an approximation of what vitamin C levels are appropriate.
The average serum vitamin C levels in the highest quartile (the one with the lowest risk of respiratory infections) was 87 µmol/L. To estimate the dose of vitamin C required to reach that level I turned to the NIH “Vitamin C Fact Sheet For Health Professionals”. From that fact sheet, I estimate that the dose needed to reach 87 µmol/L is:
150-200 mg/day for children.
200-300 mg/day for adolescents.
This is a very rough approximation, but it provides you with guidelines you can use. And those guidelines suggest you don’t need give your child a megadose of vitamin C – a chewable vitamin C supplement in the 250 mg range should be plenty.
A Holistic Approach Is Best
Bullets
I don’t want to give you the idea that vitamin C is a “magic bullet” that will protect your children from respiratory infections. For that, your children will need a strong immune system, and adequate vitamin C is just one component of a strong immune system.
For a strong immune system, a holistic approach is best. That includes:
A balanced diet composed of whole, unprocessed foods without a lot of fat and simple sugars. Unfortunately, American children currently get an average of 67% of their calories from ultra-processed foods.
Adequate sleep. The recommendations are 9-12 hours for children aged 6-12 and 8-10 hours for adolescents aged 13-18. Unfortunately, 30% of school-age children and 75% of adolescents don’t get enough sleep.
Adequate exercise. Unfortunately, children and adolescents spend far too much time on their electronic devices and too little time exercising.
Ideal body weight. Unfortunately, ultra-processed foods and lack of exercise are packing on the pounds. Almost 40% of American children and adolescents are overweight or obese.
Supplementation. Because most children eat too much ultra-processed food, I recommend a high-quality children’s multivitamin and a protein supplement to make sure they are getting the nutrients they need to build a strong immune system. That is, of course, in addition to the vitamin C supplement I mentioned above.
I recognize none of this is easy. Our son is in his 40s now, but I remember his childhood and teenage years. My only advice is to:
Pick your battles.
Be the example.
The Bottom Line
Although several recent studies have shown that vitamin C reduces the risk of respiratory infections in adults, few studies have looked at the effects of vitamin C on respiratory infections in children.
In this issue of “Health Tips From the Professor” I reviewed a study showing that vitamin C reduced the risk of respiratory infections by up to 50% in children and adolescents.
The authors concluded, “Our findings suggest that vitamin C supplementation may be potentially used for the prevention and treatment of respiratory infections among children and adolescents.”
For more information on this study, what it means for your children or grandchildren, and a holistic approach to strengthening their immune system, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
We live in a toxic world. While we are exposed to hundreds of toxic chemicals, most research in recent years has focused on two classes of toxic chemicals – phenols and parabens. They are widely used as antimicrobial agents and preservatives in personal care products, cosmetics, pharmaceuticals, and foods.
Almost 80% of personal care products contain parabens.
You find them in unexpected places like toothpaste, soap, and skin care products.
You won’t find them listed on the label of fragrances because fragrance ingredients are considered proprietary.
These chemicals are excreted in the urine, are incompletely removed during wastewater treatment, and end up in our drinking water.
With so many routes of exposure, it is no wonder our bodies have become toxic waste dumps.
Methyl and propyl parabens have been detected in the urine of 95% of adults and 99% of teenagers in this country.
Multiple phenols and parabens have been detected in the urine of most US adults.
Levels are higher in women than men because women use more personal care products.
And that is a concern because phenols and parabens:
Are endocrine disruptors.
Are associated with reproductive difficulties and developmental delays, pregnancy complications (hypertension and gestational diabetes), and birth defects.
The best evidence for these effects comes from animal studies. It has been difficult to reproduce these effects in human studies because it has been difficult to identify a large group of subjects with high enough phenol and paraben levels to give statistically significant results.
The study (JR Varshavsky et al, Journal of Environmental Health Perspectives, volume 134, Issue 8, August, 2024) I will discuss today was designed to overcome those difficulties. It determined the effect of maternal phenol and paraben levels on blood pressure and hypertension during pregnancy in a high-risk group of women – women who live in a region of Puerto Rico with 18 Superfund sites that have high concentrations of phenols and parabens in the groundwater.
How Was This Study Done?
The investigators used data from the PROTECT Center that studies exposure to environmental contamination in drinking water in Puerto Rico and its contribution to adverse pregnancy outcomes.
A total of 1,433 pregnant women between the ages of 18 and 40 (average ~25 years old) were included in the study.
They lived in the heavily contaminated Karst region in the northern part of Puerto Rico.
They were evenly split between normal and overweight + obese.
Most of them had household incomes <$30,000 per year.
Women were excluded from the study if they:
Used in vitro fertilization or oral contraceptives within 3 months of the study.
Had any known medical condition.
Were already experiencing pregnancy-related high blood pressure or gestational diabetes at the time of enrollment.
They visited clinics within the region at weeks 16-20 (visit 1) and 24-28 (visit 2) of pregnancy.
Demographic information (e.g. age, BMI, income, etc) was collected at the first visit. Blood pressure and urine samples were taken at both visits. The blood samples were analyzed for 12 phenols and parabens.
The study participants were divided into two categories according to their blood pressure.
The non-hypertensive group (<120-129 mmHg systolic blood pressure and <80 mmHg diastolic blood pressure.
The hypertensive group (130->140 mmHg systolic blood pressure and 80->90 mmHg diastolic blood pressure.
The investigators then calculated the effect of each of these phenols and parabens on the odds (risk) that the pregnant mothers would have blood pressure in the hypertensive range rather than the non-hypertensive range.
Do Phenols And Parabens Raise Blood Pressure During Pregnancy?
When the investigators combined the data from clinical visits 1 and 2, the following phenols and parabens significantly increased the odds of maternal blood pressure being in the hypertensive range:
M-PB (methylparaben) – found in cosmetics (foundations, concealers, blushes, eyeshadows, mascara, lip liners, and lipstick), skincare (moisturizers, lotions, creams, serums, face cleansers, facial treatments, and sunscreens), haircare (shampoos, conditioners, hair color and bleaching products, and styling gels), and other personal care products (shaving creams and gels, aftershave, deodorants, baby lotions, and diaper creams).
P-PB (propylparaben – found in many of the same products as M-PB (often in combination).
TCS(triclosan) – found in toothpaste, mouthwash, soaps, shampoos, deodorants, and skin creams.
TCC (triclocarban) – found in antibacterial and deodorant soaps, cosmetics, deodorants and antiperspirants.
2,4-DCP (2,4-dichlorophenol) – found in personal care products from the breakdown of triclosan.
2,5-DCP (2,5-dichlorophenol) – a breakdown product of 1,4-dichlorobenzene.
When the effect of these phenols and parabens on maternal hypertension was analyzed individually, the increased risk of maternal hypertension (high blood pressure) was 10-50%.
But when the combined effect of all the phenols and parabens was analyzed, the increased risk of maternal hypertension was almost double.
The authors concluded, “Our findings suggest that exposure to certain phenols, parabens, and their mixture may be related to maternal blood pressure differences during pregnancy, as well as to increased risk of hypertension, especially during the later stages of pregnancy.
This is important given the critical nature of cardiometabolic health during pregnancy on the future health of the both the mother and their children.”
Can Cosmetics Raise Your Blood Pressure?
At the beginning of this article I raised the question, “Can Cosmetics Raise Your Blood Pressure?”
The answer appears to be, “Yes, with a few caveats.”
1) It is the phenols and parabens in cosmetics that are responsible for the increase in blood pressure.
2) When you consider all the personal care products that contain phenols and parabens, cosmetics are just “the tip of the iceberg”
3) Most importantly, this study is what is called a “proof of concept study”. It simply shows that phenols and parabens can raise blood pressure in humans under the right conditions.
Because the investigators selected a population with very high exposure to toxic chemicals, there were enough women with high levels of polyphenols and parabens in their bodies to obtain a statistically significant association between phenols and parabens with hypertension.
The investigators also chose a population group (pregnant moms) that have a high risk of developing hypertension.
But what does this mean for you? That’s a hard question to answer.
If you are a pregnant mom with similar exposure to phenols and parabens, your risk of maternal hypertension is probably similar.
But if you’re not pregnant and your exposure is less, it is almost impossible to extrapolate your risk from these data. That’s what makes this field of research so difficult.
But let me just make these observations.
If you use personal care products, your exposure to phenols and parabens is not zero.
This, and other studies, show that we can’t just focus on the risks of individual toxic chemicals. In today’s world, we are exposed to hundreds of toxic chemicals, and their combined effects are much greater than that of any individual toxic chemical.
It’s not just blood pressure that is affected. These chemicals are endocrine disruptors that negatively affect our health in multiple ways.
In short, nobody can tell you the risks you will experience from phenol and paraben exposure, but that risk is not zero. It only makes sense to proactively limit your exposure. But how do you do that in today’s world?
How Can You Reduce Your Exposure To Phenols And Parabens?
Here are a few simple tips for reducing your exposure to phenols, parabens, and other toxic chemicals.
Start By Choosing Personal Care Products With EWG (Environmental Working Group) Verification: EWG verification means the products are free of over 500 chemicals of concern (including phenols and parabens), have full ingredient transparency (what’s in the product is on the label), and meet rigorous health and safety standards based on the latest scientific research.
Use a Water Filter: This removes contaminants, including phenols and parabens, from your tap water.
Avoid Non-Stick Cookware: Switch from non-stick (PFOA/PFAS-free) cookware to stainless steel or cast iron to avoid potential exposure to other harmful chemicals.
Keep the Air Fresh: Let in outside air to maintain good indoor air quality and reduce exposure to various environmental chemicals found in drapes, upholstery, carpets, and mattresses.
Shop Fresh and Organic: Choose fresh, organic foods and reduce your consumption of foods in plastic containers, as they may contain these chemicals.
Limit Processed Foods: Reduce or limit your intake of fast food, microwave popcorn, and takeout food.
The Bottom Line
Phenols and parabens are widely used as preservatives in cosmetics and other personal care products. Both are known endocrine disruptors and have been linked to a wide variety of adverse health consequences.
But most of the studies linking these chemicals to adverse health effects have been done with animals. It has been difficult to confirm these effects in human studies.
In this article, I describe a study with a high-risk group of women who were exposed to high levels of phenols, parabens, and other toxic chemicals. This study showed that phenol and paraben exposure increases the risk of maternal hypertension in this group of high-risk, high-exposure women.
This is what is called a “proof of concept” study. It clearly shows that phenol and paraben exposure can have adverse health effects in humans. But it is not clear how this risk extrapolates to low-risk, low-exposure populations.
In this article I discuss what the study means for you and how you can reduce your risk of exposure to phenols, parabens, and other toxic chemicals
For more information on this study, what it means for you, and how you can reduce your exposure to toxic chemicals, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
I don’t need to tell you that GLP-1 (glucagon-like peptide 1) drugs are all the rage. Total spending on GLP-1 drugs in the United States exceeded $71 billion in 2023, a 500% increase in just 5 years. There are 15 million Americans on GLP-1 drugs at any one time. And most of this increase has been driven by the weight-loss market.
Let me be clear. These drugs work. For people with poorly controlled type 2 diabetes or severe obesity-related health issues, they can be a godsend. But like any “quick fix” weight loss drugs they are overprescribed.
And when you have millions of people taking a drug, you need to take a serious look at side effects. The most frequent side effects are:
Nausea
Vomiting
Diarrhea
Constipation
Increased heart rate.
Hypoglycemia
Allergic reactions
These are side effects that aren’t life threatening and are easily detected. When someone experiences these side effects, they usually give their doctor a call, and their doctor either takes them off the drug or modifies the dosage.
However, more recent studies have identified two additional side effects that are much more troubling.
The first is depression, anxiety, and suicidal thoughts.
These are symptoms that many patients may not associate with the drug, especially if they already have these tendencies.
And the consequences can be life threatening. There have already been reports of suicides of people on GLP-1 medications.
The second is loss of muscle mass.
This is a particular concern for seniors who struggle to maintain muscle mass as they age.
And this is a silent symptom. Most seniors don’t realize they are losing muscle mass until it significantly affects their quality of life.
And, of course, the biggest drawback of GLP-1 drugs is that they are only a temporary fix. Unless someone changes their lifestyle, the weight comes roaring back as soon as they quit using GLP-1.
So. It’s no wonder some people are asking whether it is possible to increase their GLP-1 levels naturally without the side effects associated with GLP-1 drugs. I will discuss this below, but first I should review what GLP-1 is and what it does.
What Is GLP-1 And What Does It Do?
Let me start by reviewing the hormones insulin and glucagon to create a proper perspective for understanding the role of GLP-1.
Insulin: Almost everyone has heard of insulin. It is released by the pancreas whenever we eat, and blood sugar levels start to rise. Its role is to lower blood sugar levels.
Glucagon: Glucagon is less well known, but you can think of it as the Yin to insulin’s Yang. It is released by the pancreas when blood sugar levels fall and continues to be present until the next meal. Its role is to increase blood sugar levels and make sure that our cells get the food they need until the next meal.
GLP-1: GLP-1 stands for glucagon-like peptide 1. With a name like that, you might expect GLP-1 to have significant sequence homology with glucagon, bind to the same receptors, and have a similar effect on our metabolism. You would be wrong!
Both peptide hormones are derived from a much larger peptide called proglucagon. This is the only way that GLP-1 is “like” glucagon.
One portion of proglucagon is processed to give glucagon in pancreatic alpha cells. Another portion is processed to give GLP-1 in intestinal L cells. [L cells are endocrine (hormone producing cells) found in the intestinal mucosa.] There is very little sequence or structural homology between glucagon and GLP-1.
Their function is also very different. You can think of GLP-1 as a partner to insulin. It is released by intestinal L cells in response to the presence of nutrients (primarily protein, fat, and carbohydrate) in the intestine. It binds to GLP-1 receptors on the…
Pancreas to stimulate insulin release and inhibit glucagon release. This is why it helps type 2 diabetics control their blood sugar levels.
Stomach to reduce the rate of gastric emptying. This prolongs the feeling of fullness after each meal.
Small intestine to reduce gut motility, which increases transit time through the small intestine. This also prolongs the feeling of fullness after a meal. But it can also lead to gastrointestinal side effects.
Brain to turn down your “appestat”. This reduces feelings of hunger between meals. But at high doses, it can affect the brain in negative ways (anxiety, depression, and suicidal thoughts).
Can Protein Supplements Increase GLP-1?
You may be wondering, “Is it possible to increase GLP-1 levels naturally without side effects?” The answer is clearly, “Yes”. Every time you eat a meal, your GLP-1 levels increase naturally.
When you eat a meal, GLP-1 levels rise within 10 minutes and remain elevated for 1-2 hours. Then enzymes present in the bloodstream digest GLP-1 and it disappears. This is the way nature intended. There are no side effects to the natural rise and fall of GLP-1 after a meal.
And protein appears to play an important role in this process. High-protein meals result in higher and more prolonged GLP-1 levels than high-fat or high-carbohydrate meals. That’s because protein is digested to amino acids in the intestine. And some of those amino acids bind to receptors in intestinal L-cells and stimulate GLP-1 release.
You may be wondering what this has to do with protein supplements. Theoretically, protein supplements should offer the same benefit as a high-protein meal with fewer calories.
This hypothesis has been tested with a few protein supplements, and they have been shown to increase GLP-1 levels naturally. And, based on the limited data available, it appears that the increase in GLP-1 is proportional to the protein content of the supplement.
So, it appears that the answer I posed at the beginning of this article is,
Yes, it appears that protein supplements can increase protein levels naturally.
And it appears that the higher the protein content of the supplement, the greater the increase in GLP-1 levels.
However, there are many variations in the formulation of protein supplements, and we don’t know how these variations influence the effect of protein supplements on GLP-1 levels. Therefore,
We can’t yet say that all protein supplements increase GLP-1 levels equally.
When choosing a protein supplement, you should ask for clinical studies with their product showing it increases GLP-1 levels.
What Does This Mean For You?
If you can raise your GLP-1 levels naturally with high-protein meals and protein supplements, you might be asking, “What makes the GLP-1 drugs different?” To understand the answer to that question, you first need to know what GLP-1 drugs are.
GLP-1 drugs mimic the natural GLP-1 peptide.
However, GLP-1 drugs have been genetically modified to make them resistant to enzymatic digestion. They can stay in the bloodstream for up to 24 hours.
This is what makes them so effective as weight loss drugs. But it’s not nice to fool with mother nature. This is also why they have side effects.
And let’s remember that while GLP-1 drugs are effective, you will need to take them for the rest of your life unless you change your diet and lifestyle. And with long-term usage of the drugs, you are likely to experience one or more of their side effects at some point.
So, if you are willing to change your diet and lifestyle, it may be worthwhile looking at increasing your GLP-1 levels naturally. The effect may not be as strong as with the GLP-1 drugs, but it may help you suppress your appetite enough to successfully implement your lifestyle changes. You have lots of options.
Every time you eat a meal your GLP-1 levels increase. And the bigger the meal, the bigger the increase. But the bigger the meal, the greater the calories. So, that’s not an optimal way to increase GLP-1 levels.
That’s where protein supplements come in.
And since you are trying to maximize GLP-1 levels with the minimum calories, I recommend a 20–40-gram protein supplement with a minimum of carbohydrate and fat. Just be sure the manufacturer has done a clinical study to demonstrate their protein supplement raises GLP-1 levels.
The Bottom Line
In this article I asked the question, “Can protein supplements increase GLP-1 levels naturally without the side effects of GLP-1 drugs?” The answer is, “Yes”. In this article I tell you:
What GLP-1 is and what it does.
Why GLP-1 drugs have side effects.
How protein supplements can raise your GLP-1 levels naturally without the side effects of GLP-1 drugs.
For more details read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
In 2016 the New York Times ran an article with the title, “Can You Get Too Much Protein?” The article asserted that most Americans were getting too much protein in their diet and that protein supplements were useless and perhaps dangerous.
At the time I wrote a “Health Tips From the Professor” article summarizing recent research showing that many people needed more than the RDA for protein and that those people were often consuming too little, rather than too much, protein.
In the 9 years since then the evidence that many Americans may not be getting enough protein has only gotten stronger.
The standard for protein intake used to be a “one size fits all” recommendation of 46g gm/day for women and 56 gm/day for men with slight increases recommended for pregnant and lactating women. Today we know:
That standard was based on outdated methodology from the 1930’s. Recent studies suggest protein intake should be at least 50% higher.
That standard was based on studies with healthy, sedentary adults (the adult “couch potato” crowd). Protein requirements are significantly higher for anyone who doesn’t fit that description.
We used to think in terms of total daily protein intake. Today we know that:
Protein intake should be divided equally between the 3 primary meals.
Protein quality is important. Protein requirements should be increased if low-quality proteins are consumed.
We used to worry that high protein intake might damage your kidneys. Today we know that:
Protein intake does not cause kidney disease. It is not a concern as long as hydration is adequate and excess alcohol is avoided.
Protein intake is only a concern if someone has kidney disease.
Her book is focused on helping each of us create adequate healthy muscle mass. She says, “Adequate muscle mass is essential for health and longevity. And muscle is the only organ over which we have voluntary and complete control.”
Of course, adequate muscle mass requires both exercise and adequate protein. Dr. Lyon covers both in her book, but exercise is not my expertise, so I will only cover adequate protein intake in this “Health Tips From the Professor” article.
In her book, Dr. Lyons details recent research on the amount of protein needed to optimize muscle mass. Dr. Lyon was the one who alerted me to the fact that the current protein RDA is based on outdated methodology from the 1930’s and that actual protein needs are much higher.
Dr. Lyon concludes that most Americans are not consuming enough protein to optimize their muscle mass and that adequate protein intake is essential for longevity, metabolic function, and quality of life. Specifically, she says that optimal muscle mass:
Improves strength and mobility.
Improves blood sugar control.
Decreases blood triglyceride levels.
Strengthens the immune system.
Improves bone mineral density and strength.
Reduces all-cause mortality (risk of dying) and morbidity (risk of disease).
I will use the latest science on protein needs described in her book and in recently published clinical studies to answer the important question, “How much protein do you need?” But first I want to help you understand the dynamics of protein metabolism.
The Dynamics Of Protein Metabolism
Most people associate muscle mass with strength and endurance. Many understand the important role muscle mass plays in burning off excess calories and keeping us slim. But few people understand the important role that muscle protein plays in our everyday energy metabolism.
Whenever we eat a meal containing protein, we store some of the protein we eat as increased muscle mass, especially when protein intake is coupled with exercise. But muscle protein plays other very important functions. It is a precious resource.
The synthesis of new muscle in the fed state is driven by:
Insulin, which is released into the blood stream whenever we eat a meal.
Exercise because it makes muscle more sensitive to the effects of insulin.
The amino acid leucine, which is most abundant in high quality protein sources.
In the fed state most of our energy is derived from blood glucose. This is primarily controlled by insulin. As blood glucose levels fall, we move to the fasting state and start to call on our stored energy sources to keep our body functioning. This process is primarily controlled by a hormone called glucagon.
In the fasting state most tissues easily switch to using fat as their main energy source, but…
Red blood cells and a few other tissues in the body are totally dependent on glucose as an energy source.
Our brain is normally dependent on glucose as an energy source, and our brains use a lot of energy. [Note: Our brain can switch to ketones as an energy source with prolonged starvation or prolonged carbohydrate restriction, but that’s another story for another day.]
Because our brain and other tissues need glucose in the fasting state, it is important to maintain a constant blood glucose level between meals.
Initially, blood glucose levels are maintained by calling on carbohydrate reserves in the liver.
But because those reserves are limited, our body starts to break down muscle protein and convert it to glucose as well – even in the normal dinner/sleep/breakfast cycle.
Simply put, in addition to its other important roles in the body, muscle protein is also an energy store. You can think of it like a bank.
When we eat, we make a deposit to that energy store. Between meals we make a withdrawal from that energy store. When we are young the system works perfectly. Unless we fast for prolonged periods of time, we are always adding enough muscle protein in the fed state to balance out the withdrawals between meals.
But there are many physiological situations where protein metabolism becomes unbalanced, either because protein breakdown is accelerated or because protein synthesis is diminished. In each of those situations, our protein needs are increased.
I will describe each of these situations and how they affect our protein needs in the section below.
How Much Protein Do You Need?
The Coach Potato Group: If this is you, I won’t be judgmental. But I highly recommend you read Dr. Lyon’s book. It may just inspire you to increase your fitness level and your protein intake.
As I said before the standard RDA recommendation for the coach potato group is 46 gm/day for women and 56 gm/day for men. That’s based on 0.36 grams of protein per pound of body weight and assumes that women weigh around 127 pounds and men weigh around 155 pounds.
There are two major problems with the standard protein RDAs:
1) The protein RDA should not be a “one-size-fits-all” recommendation. The standard used to calculate the RDA is based on weight. If you are a woman weighing 127 pounds or a man weighing 155 pounds, you are to be congratulated. But in today’s world the average woman weighs 170 pounds, and the average man weighs 201 pounds.
That means the average protein requirement should be 61 gm/day for women and 72 gm/day for men.
And that’s just the average. Your protein requirement is based on your weight.
2) As I mentioned earlier, the 0.36 gm/pound standard is based on outdated methodology from the 1930’s. Based on current technology, Dr. Lyon says the standard should be closer to 0.54 gm/pound.
If you use that standard and use the current average weight for men and women, the average protein requirement for the couch potato group is closer to 91.5 gm/day for women and 108 gm/day for men.
And since protein intake should be divided equally between meals, that amounts to 30 gm/meal for women and 36 gm/meal for men. If you weigh significantly more or less than the average American, you should adjust your intake accordingly.
The Over 50 Group: When we are young muscle protein deposits in the fed state and muscle protein withdrawals during the fasting state are in balance. And if we add exercise and increase our protein intake, it’s pretty easy to increase our muscle mass.
But once we reach our Golden Years things start to change. Muscle protein synthesis becomes less efficient. We need to increase the intensity of our workouts and increase our protein intake just to maintain our muscle mass.
If we fail to do that, we gradually lose muscle mass as we age, a process referred to as sarcopenia. Between 50 and 60 we lose 5-8% of our muscle mass, and the rate that we lose muscle accelerates with each subsequent decade. And that loss of muscle mass has severe consequences. For example:
It interferes with daily activities like playing with our grandchildren and engaging in activities we love.
It decreases our metabolic rate which increases our risk of obesity and obesity-related diseases.
It increases our risk of falls.
In short, our quality of life is diminished, and we become unhealthy and frail.
Dr. Lyon describes the training program needed to prevent sarcopenia as we age in her book Forever Strong. But we also need more protein.
On average older adults need around 35 – 45 gm of protein per meal to prevent sarcopenia. There are not enough published studies for me to provide more specific recommendations. But here are some guidelines:
If you are at ideal weight and in your 50’s or 60’s, you can probably do well at the lower end of the range.
If you are overweight or in your 70’s or 80’s, you should probably aim for the upper end of the range.
I recommend getting a body composition test on an annual basis and adjusting your exercise and protein intake based on your change in muscle mass. My doctor has a simple device for measuring my body composition as part of my annual physical. If your doctor doesn’t have a device like that, find out who does in your community.
The Weight Loss Group: If you are actively trying to lose excess weight, I congratulate you. But the sad fact is that up to 35% of weight loss on most diets comes from muscle, not fat.
That’s because your body interprets caloric restriction as starvation and increases the rate of protein breakdown.
But you can prevent that by adding resistance training to your diet plan and increasing your protein intake. By increasing your protein intake from 15% of calories (which is what most Americans get) to 30% of calories, you can rebalance muscle metabolism by increasing muscle protein synthesis. When you do this, you can reduce muscle loss to less than 10% of weight loss.
You may be wondering, “Why set the recommendation as a percentage of calories rather than gm/pound or gm/meal”. The answer is simple. Your caloric intake changes significantly you are on a diet, so expressing protein as a percentage of calories makes more sense.
For example, 30% of calories on a 1,000-calorie diet translates into 25-30 gm/meal. You might look at that recommendation and say, “That’s less than you recommended for the couch potato who is not trying to lose weight.” My answer would be, “Yes, but the couch potato is eating 2-3-times more calories.
So, the recommendation that’s easiest to understand if you are trying to lose weight is to aim for 25-30 gm of protein/meal/1,000 calories per day.
Adjust your protein intake per meal based on the daily calories allowed on your diet.
And if you are on a diet that restricts the kinds of food that you can eat or the amount of time you can eat, track your actual caloric intake for a few days. The “hidden secret” behind those diets is that most people eat fewer calories because of the restrictions.
Final thought: The latest data suggest that GLP-1 drugs accelerate the muscle loss associated with dieting. This is a significant concern, especially for people over 50. Some experts are recommending as much as 35-50 gm of protein/meal if you are using a GLP-1 drug to aid your weight loss.
The Fitness Group: The question I get most often from the fitness group is, “How much protein do I need after my workout to maximize recovery and muscle gain?” This has been well researched, and the answer is age dependent.
If you are in your 30’s, most experts recommend 15-20 grams of protein after your workout.
If you are in your 60s, most experts recommend 30-35 grams of protein after your workout.
While precise recommendations are not available for every age, you can extrapolate from these numbers.
Does Protein Quality Matter?
I’m often asked whether all proteins are equally effective at building muscle mass or does protein quality matter? The answer is, “Yes. Protein quality matters, but not in the way that we have thought about it in the past.”
We used to think that protein quality was measured by the balance of all the essential amino acids. While balance is important, the increase in muscle mass is driven primarily by the amino acid leucine. That’s because leucine is the only amino acid that directly stimulates muscle protein synthesis.
Simply put, proteins that are high in leucine are used more efficiently by our bodies to increase muscle mass. In fact, Dr. Lyon measures protein quality solely based on its leucine content.
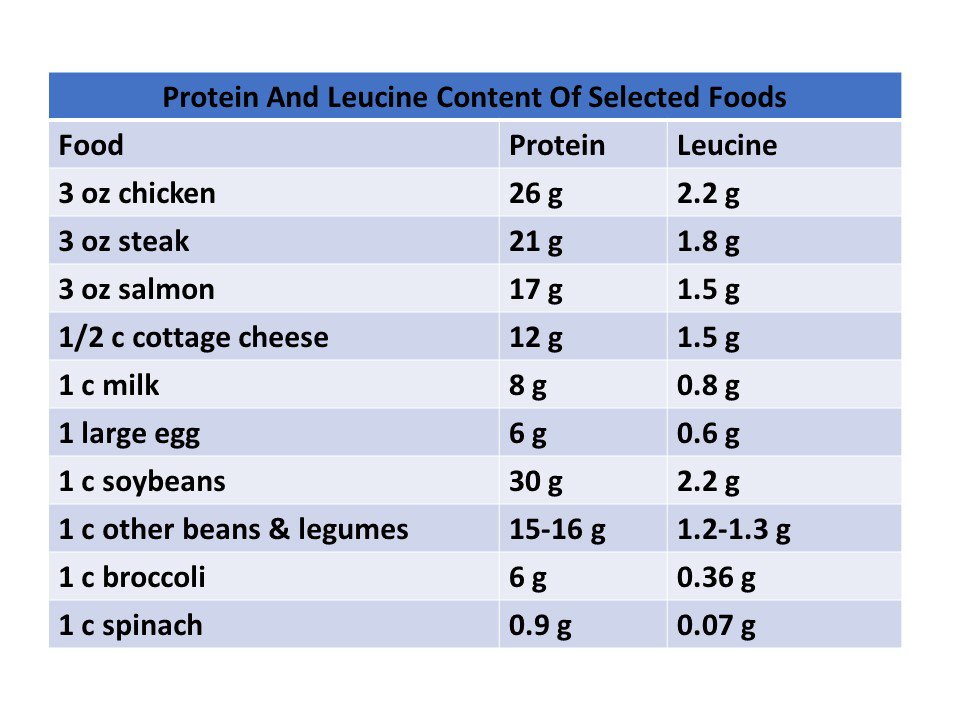
Many studies have looked at the optimal amount of leucine content in protein. The numbers vary somewhat from study to study, but they average around 1 gram of leucine for every 10 grams of protein.
If you look at the leucine contents of various proteins, it is clear that a 1:10 ratio is primarily found in animal proteins. Soybeans are the only vegetable protein source that comes close.However, there are many health reasons for consuming a primarily plant-based diet. Dr. Lyon doesn’t tell her patients to avoid plant proteins. But if they are consuming primarily plant proteins, she recommends that they increase their protein intake by 35-45%, so they will be getting enough leucine to maximize muscle protein synthesis.
What Role Do Protein Supplements Play?
Remember that New York Times article that said protein supplements were useless and perhaps dangerous? That’s outdated advice. In fact, you should view protein supplements as essential for reaching your protein goals.
That’s because our protein intake needs to be divided equally between our 3 major meals, but that’s not how we eat. Most of us have no trouble getting 30-40 grams of protein at dinner, but…
We only get around 15 grams of protein at breakfast, and…
15-20 grams of protein at lunch.
But that’s assuming we eat a typical breakfast or lunch. If we eat…
An unhealthy breakfast of croissants and coffee or a healthy breakfast of cornflakes, skim milk, and fruit slices, we only get around 6 grams of protein.
A healthy green salad for lunch, we may get as little as 2 grams of protein.
A recent study has shown that adding a protein supplement to your low protein meals can help you increase your muscle mass in as little as 24 weeks.
What Does This Mean For You?
Protein is your longevity nutrient. My advice is:
Use the information in this article to set your protein goals (Talk with your doctor first if you have any health issues that may limit your protein intake).
Use a simple protein tracker to identify your low-protein meals.
Add additional protein foods or supplements to your low-protein meals to bring your protein up to recommended levels.
Focus on high-leucine protein foods and supplements. (If you eat more plant protein than animal protein, as I do, increase your recommended protein intake by 35-45% to make sure you are getting the leucine you need to maximize your muscle mass.)
As for what kind of protein supplement, I recommend a plant protein supplement with added leucine.
The Bottom Line
In her book, “Forever Strong”, Dr. Gabrielle Lyon says, “Adequate muscle mass is essential for health and longevity. And muscle is the only organ over which we have voluntary and complete control.” She goes on to state that the current RDAs for protein intake are outdated. And if we look at protein needs based on the latest research, most Americans aren’t getting enough protein in their diet to achieve adequate muscle mass.
In this article, I summarize her findings. And based on the latest research, I provide protein intake recommendations for:
Adult couch potatoes.
Fitness enthusiasts.
People over 50.
People who are trying to lose weight.
I also discuss protein quality and protein supplements.
For more information on these topics and what they mean for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
There are lots of multivitamin-multimineral products in the marketplace. Every company must differentiate their product from the competition to win their market share. When that differentiation is based on quality, purity, and clinical proof the product works, I am all for it. May the best company win.
However, the pressure to win market share is intense. Quality controls and clinical studies are expensive. All too often companies try to differentiate their multivitamin-multimineral products based on marketing hype and/or worthless ingredients that subtract money from your wallet without adding anything of value to your health.
With so many claims and counter claims in the marketplace, it has become almost impossible for the average consumer to know which claims are true and which are false. Everyone wants to get the best multivitamin-multimineral for their health at the least possible cost. Perhaps that is why I am so frequently asked for guidance on how to choose the best multivitamin.
In this week’s article, I will give you 6 tips you can use to select the multivitamin-multimineral product that is best for you. I will tell you what to look for in a good multivitamin and which marketing claims you should just ignore.
But first, we need to look at how nutritional standards are set.
How Are Nutritional Standards Set?
The standards for nutritional supplements are set in a two-step process.
Step 1: In the first step, The Institute of Medicine (IOM) of the National Academies of Sciences selects a committee of experts called the Food and Nutrition Board to set standards for a specific set of nutrients. They set 3 kinds of standards:
Recommended Dietary Allowances or RDAs are the average daily dietary intake level sufficient to meet the nutrient requirements of nearly all (97-98 percent) healthy individuals in a group.
Adequate Intakes or AIs are established when evidence is insufficient to develop an RDA and are set at a level assumed to ensure nutritional adequacy.
Where toxicity is a potential concern, Tolerable Upper Limits or ULs represent the maximum daily intake unlikely to cause adverse health effects.
Just to confuse things, all three standards are part of what is called Dietary Reference Intakes or DRIs.
Step 2: The DRIs are specific for age, gender, pregnancy & lactation. It would be hopelessly complicated to use DRIs for nutrition labels on foods and supplements. Therefore, the FDA sets a Daily Value (DV) for the purposes of food and supplement labeling. Originally, DVs were set based on the highest DRI for a specific nutrient. However, currently the DV is an average of DRIs for adults and children 4 years and older. It is not identical to the RDA or DRI for any specific group, but it is a useful standard for supplement labels.
With this information in mind, let’s get back to the 6 tips for choosing the best multivitamin.
#1: Good Product Design Matters
Comparing nutrition labels on multivitamin-multimineral supplements can be tricky. Some supplements only provide 5-10% of the Daily Value (DV) for some nutrients. Are those nutrients unimportant? Some supplements provide hundreds or thousands % of the DV for other nutrients. Is more better?
Often companies will quote some random scientist or one or two clinical studies to support the mix of nutrients they include in their multivitamin-multimineral supplement. Don’t fall for their marketing hype.
The only valid nutritional standards for multivitamin-multimineral products in the United States are the DV standards set by the Food & Nutrition Board of the Institute of Medicine. They are the standards you should look for in evaluating nutrition labels.
That’s because the National Academies of Sciences is the real deal. The National Academies represents the top 1-2% of scientists in the country. To be selected to the National Academies you must be nominated by an Academy member and voted on by the entire Academy. Selection is based on your research contributions over decades. (No, I am not a member of the Academy, but thanks for thinking that question).
The Institute of Medicine of the National Academies of Sciences selects the best of the best to serve on the Food and Nutrition Board. They are world renowned experts who review all the pertinent literature (not just one or two studies) They decide on which nutrients are essential and how much of them we need.
It always amazes me that some companies pretend they know more than the Food and Nutrition Board. It amazes me even more that some people believe those companies.
With that in mind, this is what to look for when comparing nutrition labels:
The FDA has set Daily Value (DV) recommendations for 24 vitamins and minerals (23 if the supplement is for adult men or postmenopausal women and does not contain iron). Make sure your multivitamin-multimineral has all 24. Count them. If a company leaves out an essential nutrient, they are not required to list it on the label.
The Food and Nutrition Board has classified several other nutrients as essential but does not feel there have been enough studies to establish a DRI. Without a DRI, the FDA cannot set a DV. Those nutrients are represented with a “dagger” symbol on the label with the footnote “Daily Value not established”. These can be useful additions to a multivitamin-multimineral supplement, provided they are not present in excess.
Ignore anything companies list on their nutrition labels that does not have a %DV value or a “dagger” symbol. This is often just marketing hype. In some cases, the ingredients have no proven benefit. In many other cases, it’s just not possible to put enough of them in a multivitamin-multimineral tablet to provide any real benefit.
#2: Look For Balance
This is another area in which we need to be guided by the recommendations of the Food and Nutrition Board of the Institute of Medicine. One of the reasons many experts recommend that people get their vitamins and minerals from foods rather than from supplements is because many supplements are unbalanced. That’s a problem because there are many cases in which too much of one nutrient can interfere with the absorption or metabolism of related nutrients. For example,
Zinc and copper compete for absorption. For best absorption and maximal utilization by the body, the zinc to copper ratio should be close to 1:1 based on DV.
B vitamins should be in balance. Look for a multivitamin-multimineral supplement that provides100-200% of the DV for all 8 essential B vitamins. (The levels can be higher in a B Complex supplement, but they should still be in balance.)
Some manufacturers will leave out the expensive B vitamins and load up on the cheap ones. This saves them money. It also allows them to use marketing terms like “mega” or “super”. A supplement that provides 50% or less of the DV for some B vitamins and 1,000% or more of the DV for others is ridiculous. There is absolutely no rationale for a ratio like that except to mislead consumers.
As for the other nutrients in multivitamin-multimineral supplements, they should not be significantly below 50% or significantly above 250% of the DV.
Calcium, magnesium, and phosphorous are a special case. They are bulky, so many manufacturers only provide 5-10% of them in their multivitamin-multimineral supplements. This is not ideal because many of the nutrients in a multivitamin-multimineral supplement are required for optimal utilization of calcium and magnesium in bone formation.
Many Americans get only 50% of the DV for calcium and magnesium in their diet. Thus, it makes good sense to provide 30-50% of the DV for calcium and magnesium in a multivitamin multimineral supplement. Most Americans get close to the DV for phosphorous from their diet, so the amount of phosphorous in a supplement is not particularly important.
#3: Don’t Fall For The Hype
In their attempts to differentiate themselves, many companies claim that they use a more natural or a better utilized form of the vitamin or mineral than their competitors. Ignore those claims. They are just marketing hype. For example,
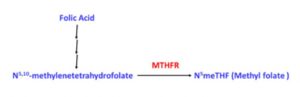
In previous issues of “Health Tips From the Professor” I have debunked the claims that folate and methyl folate are more natural, safer and more effective than folic acid. The claims that alternate chemical forms of other vitamins are more natural, safer, and more effective are equally bogus.
The claims by some manufacturers that they use a form of calcium that is more readily absorbed are not just misleading. That is the wrong question. Calcium in our bloodstream can do bad things (like calcification and hardening of the arteries) if it is not quickly utilized for bone formation.
Thus, the important question is how well the calcium is utilized for bone formation. Look for clinical studies showing that the calcium in their multivitamin-multimineral supplement is efficiently utilized for bone formation rather than hype about how quickly it gets into the bloodstream.
There is a good reason that many supplement companies continue to use ingredients like folic acid for B9, cyanocobalamin for B12, pyridoxine for B6, etc. All of them are supported by hundreds of clinical studies showing that they are safe and effective. I have no issue with companies choosing to use different forms of these vitamins. Just don’t fall for their hype that the forms they are using are somehow more natural, safer or more effective than the traditionally used forms of the same vitamin.
#4: Don’t Fall For Buzz Words
Pinochio
Some manufacturers attempt to differentiate their products by claiming they are natural, organic, non-GMO, or are made from food. The companies are attaching buzz words to their product that they know resonate with the American people. Don’t believe them. Those claims are all bogus. They are marketing hype. For example,
There is no standard for “natural” so companies are not required to provide any evidence to back up their claim. If they claim that their product is natural, ask for a detailed list of the source and processing method for all their ingredients. If they are unwilling or unable to provide you with that information, don’t believe their claim of natural.
“Organic” certification for a supplement simply means that ingredients come from crops raised using organic methods. It is no guarantee of purity. Organically grown crops can still be contaminated if the air, soil or water is contaminated from any nearby pollution source. For example, ground water pollution is the major source of heavy metal contamination often seen in rice-derived ingredients. It is far more important to select your supplement based on rigorous quality control standards that assure it is pure than to rely on “organic” on the label.
A “non-GMO” designation is useful for foods and for protein, but it is meaningless for the ingredients in a multivitamin-multimineral supplement. Those ingredients have been extensively purified. They contain no genetic information. They are chemically indistinguishable from purified ingredients obtained from GMO sources. If you would like more detailed information about the GMO controversy, I have provided a balanced perspective on GMO in a video.
Claims by some companies that their vitamins are derived from foods are completely bogus. That is a physical impossibility. For example, let’s look at what it would take to provide the DV for just 3 of the nutrients in a single multivitamin pill, assuming they started with the best food sources of those 3 nutrients:
It would take 1 cup of cooked lentils, 2 cups of cooked spinach, or 4 cups of cooked broccoli to provide the DV for folic acid.
It would take 1 cup of sunflower seeds, 1.5 cups of pistachio nuts, or 7 ounces of cooked tuna to provide the DV for vitamin B6.
It would take 5 ounces of cooked chicken breast, 1 cup of peanuts, or 6 cups of green peas to provide the DV for niacin.
That’s just 3 nutrients and one multivitamin tablet. You do the math. If they lie to you about their vitamins coming from food, they will probably lie about other things as well.
#5: Don’t Fall For Scare Tactics
Some companies try to scare you into buying their products by claiming their competitors are using unsafe ingredients. These claims are usually bogus, but it is useful to understand where this misinformation comes from.
There is a lot of unfounded hysteria on the internet about product ingredients. Much of this hysteria has been fueled by a few well-known bloggers. I believe their intentions were pure in the beginning. They started by warning the public about truly dangerous ingredients like artificial colors, flavors, preservatives and sweeteners.
However, blogging has a dark side. To capture a large audience, your blog posts need to be sensational every week. As the weeks go by it becomes harder and harder to find subject matter that is both sensational and accurate. That’s when some bloggers go over to “the dark side”.
They become more concerned about the size of their audience than the accuracy of the information they post. They start vilifying ingredients that are perfectly safe as long as the manufacturer purifies them correctly and tests them for purity. These are ingredients which might be of concern for products made by a company with poor quality controls but pose no concern for products made by a company with high quality control standards. In other words, they should not be spreading hysteria about the ingredient. They should focus on some of the real quality control issues in our industry.
To help you sort through all the hysteria about product ingredients, I have previously published a two-part series on ingredients in which I sorted through the claims and divided common ingredients into the good, the bad, and the ugly.
#6: Demand Proof
This is the most important tip of all. Many companies make wild claims about their products but feel no need to back up their claims. Ignore their hype and demand they give proof to back up their claims.
If they claim their products are pure, ask how many quality control tests they run on their products.
If they claim their products work, ask for proof. Ask for clinical studies…
That have been done with people, not with animals, cell culture, or test tubes*
That have been published in peer-reviewed scientific journals.
That have been done with their product, not studies done with another product.
*Animal, cell culture and test tube studies are valid if they are used to identify a potential mechanism of action but should not be cited as proof the product works. For ethical reasons, I prefer companies that do not use animal studies.
The Bottom Line
Everyone would like to get the best multivitamin-multimineral for their health at the least possible cost. However, there are lots of multivitamin-multimineral products in the marketplace. The pressure to win market share is intense. Quality controls and clinical studies are expensive. All too often companies try to differentiate their multivitamin-multimineral products based on marketing hype.
With so many claims and counter claims in the marketplace, it has become almost impossible for the average consumer to know how to choose the best multivitamin-multimineral product. In this week’s article, I have given you 6 tips you can use to select the multivitamin-multimineral product that is best for you. I have told you what to look for in a good multivitamin and which marketing claims you should just ignore. In summary:
Start with the nutrition label. A good multivitamin-multimineral supplement should contain all 24 essential nutrients recommended by the Food and Nutrition Board of the Institute of Medicine (23 if the supplement is without iron). Anything else is probably marketing hype.
Make sure the nutrients are in the correct balance. Again, your evaluation should be guided by the Institute of Medicine.
Don’t fall for the hype. Many companies claim that they use a more natural, safer, or better utilized form of certain vitamins or minerals than their competitors. Ignore those claims. They are usually just marketing hype
Don’t fall for buzz words. Some companies attempt to differentiate their products by claiming they are natural, organic, non-GMO, or are made from food. The companies are attaching buzz words to their product that they know resonate with the American people. Don’t believe them. Those claims are all bogus. They do nothing to improve your health. They are marketing hype.
Don’t fall for scare tactics. Some companies try to scare you into buying their products by claiming their competitors are using unsafe ingredients. These claims are usually bogus.
Demand poof. This is the most important tip of all. Many companies make wild claims about their products but feel no need to back up their claims. Ignore their hype and demand they give proof to back up their claims.
If they claim their products are pure, ask how many quality control tests they run on their products.
If they claim their products work, ask for proof. Ask for clinical studies…
That have been done with people, not with animals, cell culture, or test tubes.
That have been published in peer-reviewed scientific journals.
That have been done with their product, not studies done with another product.
For more details about each of those tips, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 45 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
Osteoporosis is one of the dreaded diseases associated with aging.
Over 50% of women and 25% of men will develop osteoporosis in their lifetime.
And the risk of osteoporosis is highest for Caucasians.
Over 40% of white women and 13% of white men will develop an osteoporotic fracture in their lifetime.
And osteoporotic fractures can be deadly. Bone fractures increase the risk of death 3-5-fold within the next few months. Moreover, the quality of life is diminished, and the risk of death is elevated for years after the fracture occurs.
So, if you are like many people, you are doing all you can to keep your bones strong so you will minimize your chances of developing osteoporosis. You probably even have a check list:
Resistance exercise (strengthens the bones you pull on)……Check
Walking (strengthens hip and leg bones)………………………Check
Adequate calcium & vitamin D (essential for strong bones)…Check
Magnesium & vitamin K (also important for strong bones)…..Check
Adequate protein (Muscle pulling on bone strengthens it)…..Check
Adequate omega-3s………………………………………………What!!!
You probably didn’t know about omega-3s. But recent research suggests they may also play a role in building strong bones and preventing osteoporosis. For example, studies show that omega-3s may influence bone metabolism by:
Enhancing absorption of calcium from the intestine.
Reducing the rate at which bone is broken down.
Increasing the rate at which new bone is built.
But large-scale population studies showing that omega-3 intake influences the risk of developing osteoporosis are lacking. The study ( Z Liu et al, Frontiers In Nutrition, 11: 1467559, 2023) I am discussing today was designed to fill that gap.
But before I describe the study, I should give you a quick review of bone metabolism.
Biochemistry 101: Bone Metabolism
To truly understand osteoporosis and how to prevent it, you need to know a bit about bone metabolism. We tend to think of our bones as solid and unchanging, much like the steel girders supporting an office building. Nothing could be further from the truth. Our bones are dynamic organs that are in constant change throughout our lives.
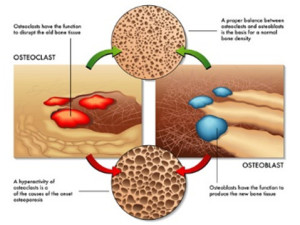
Cells called osteoclasts constantly break down old bone (a process called resorption), and cells called osteoblasts replace it with new bone (a process called accretion). Without this constant renewal process our bones would quickly become old and brittle.
In short, our bones are not inert. They are in constant flux. If we exercise regularly and get enough calcium, vitamin D, magnesium, and vitamin K from our diet, bone metabolism looks like this as we age.
When we are young, osteoblast activity predominates, so accretion (the bone building process) exceeds bone resorption, and our bones grow in size and density.
When we are adults, osteoblast and osteoclast activity are in balance. Thus, bone accretion and resorption are in balance, and our bone density stays constant. The top portion of the picture above depicts what happens when osteoclast and osteoblast activity are in balance.
However, as we age osteoclast activity predominates, and we start to lose bone density. Eventually our bones look like Swiss cheese and break very easily. This is called osteoporosis. The bottom portion of the picture depicts this.
We should also think of our bones as calcium reservoirs. We need calcium in our bloodstream 24 hours a day for our muscles, brain, and nerves to function properly, but we only get calcium in our diet at discrete intervals. Consequently:
When we eat our body tries to store as much calcium as possible in our bones.
Between meals, we break down bone material so that we can release the calcium into our bloodstream that our muscle, brain & nerves need to function.
If we lead a “bone healthy” lifestyle, all of this works perfectly. We build strong bones during our growing years, maintain healthy bones during our adult years, and only lose bone density slowly as we age – maybe never experiencing osteoporosis. We always accumulate enough calcium in our bones during meals to provide for the rest of our body between meals.
I should note that this is the current paradigm for bone metabolism. The study I am discussing today is asking whether omega-3 fatty acids should also be considered as part of a bone-healthy lifestyle.
How Was This Study Done?
The investigators used data from NHANES (National Health And Nutrition Examination Survey), an ongoing study to assess the health and nutritional status of adults and children in the United States. Specifically, this study combined data from participants from the 2005-2010, 2013-2014, and 2017-2018 NHANES surveys.
The participants included in the survey:
Were greater than 50 years old.
Had completed two 24-hour dietary recall surveys to determine the omega-3 content of their diet (The average omega-3 intake of the two surveys was used for this study).
Had a bone mineral density (BMD) test performed using dual-energy X-ray absorptiometry (DXA) scans.
Participants were excluded from the study if they had incomplete diet or bone mineral density data or if they had a disease that affects bone metabolism.
A total of 8,889 participants were included in the study. They were divided into 3 categories based on their bone density:
Normal bone density (4,421 participants)
Osteopenia (3,952 participants)
Osteoporosis (516 participants)
Finally, the participants were divided into quartiles based on their omega-3 intake, and omega-3 intake was correlated with bone density.
Are Omega-3s Needed For Strong Bones?
The study results were as follows:
Omega-3 intake was inversely related to bone density. Simply put, that means:
The highest intake of omega-3s was observed in the group with normal bone density, and…
The lowest omega-3 intake was observed in the osteoporosis group.
When the participants were divided into quartiles based on their omega-3 intake:
Participants with the highest omega-3 intake were 29% less likely to develop osteoporosis than participants with the lowest omega-3 intake.
When the investigators looked at subgroups, they found stronger effects of omega-3s on osteoporosis risk for women, people under 60, and non-smokers. Specifically:
Women with the highest omega-3 intake were 35% less likely to develop osteoporosis.
People under 60 were 49% less likely to develop osteoporosis.
Non-smokers were 36% less likely to develop osteoporosis.
The investigators concluded, “This study demonstrates a significant inverse relationship between dietary omega-3 fatty acid intake and osteoporosis risk, suggesting omega-3s play a crucial role in bone health. However, further longitudinal studies are needed to confirm these studies and refine dietary recommendations for osteoporosis prevention.”
Why Are Omega-3s Needed For Strong Bones?
You are probably thinking,
“Calcium and magnesium are part of bone structure. Vitamin D and vitamin K facilitate the incorporation of calcium into bone. So, it is logical that these nutrients would be important for strong bones.”
“But what role do omega-3s play? They aren’t incorporated into bone, and they don’t affect calcium metabolism.”
Here is what the authors said about that:
Omega-3s are anti-inflammatory. They decrease production of the pro-inflammatory cytokines that stimulate osteoclasts – the cells that break down bone.
EPA and DHA are also converted to prostaglandins that stimulate osteoblasts – the cells that build new bone.
Finally, the authors said, “Omega-3 fatty acids, especially EPA and DHA, have been shown to enhance calcium absorption in the gut – a process crucial for maintaining optimal bone mineral density…Omega-3s …do this by altering the lipid composition of cell membranes, thereby affecting calcium channels and enhancing calcium availability for bone tissue.”
Let me help you understand that statement.
While we might think of our cell membranes as rigid structures, they are quite fluid. The closest analogy I can think of is a large lake. You may not see any waves or ripples, but if a leaf drops on the surface it doesn’t stay in one place. It moves. We can think of calcium channels in our membrane like leaves on the water. They move across the cell membrane.
How fast they move depends on the fluidity of the cell membrane. This is determined by the lipids (fats) in the cell membrane, which in turn is determined by the fats in our diet. This is the one case where it is literally true that we are what we eat.
When we have lots of saturated fats in our cell membranes, fluidity is low, and calcium channels move slowly across the membrane.
When we have omega-3 fats in our cell membrane, fluidity is high, and calcium channels move quickly across the cell membrane.
Calcium channels work best when they cluster together, and this works best with highly fluid, omega-3-rich cell membranes.
What Does This Mean For You?
This study strongly suggests that omega-3s play a role in bone health, and they may be important for reducing our risk of osteoporosis. The authors concluded, “The findings suggest that omega-3 fatty acids play a critical role in bone health, supporting the need for dietary recommendations that encourage omega-3 consumption as a preventative measure against osteoporosis.”
However, this is the first study of its kind, which is why the authors said, “Further longitudinal studies are needed to confirm these findings.”
However, my biggest concern with the study is that it did not include information on the intake of the other nutrients essential for bone health (calcium, vitamin D, magnesium, and vitamin K). We don’t know at present the importance of omega-3s for preventing osteoporosis relative to dietary intake of other bone-healthy nutrients. For example:
Are omega-3s important for bone health when intake of calcium and/or the other bone-healthy nutrients are low?
Or are omega-3s equally important for bone health under all conditions?
However, the good news is that omega-3s have many proven health benefits such as heart health, controlling blood pressure, and reducing inflammation. If they are also important for bone health, we can consider it an unexpected benefit.
With that in mind, there are two important takeaways for you:
Omega-3s were most effective at preventing osteoporosis in people under 60. That is entirely consistent with what we know about preventing osteoporosis. The best prevention strategy is to build strong bones while you are young and maintain strong bones as long as possible in your adult years.
The optimal reduction of osteoporosis risk in this study was seen with an omega-3 intake of 1.86 g/d. While more studies are needed to define the optimal dose of omega-3s for reducing osteoporosis risk, this dose is within the “sweet spot” for the other omega-3 benefits I mentioned.
The Bottom Line
A recent study asked whether omega-3 fatty acids reduce the risk of osteoporosis.
The study found:
Omega-3 intake was inversely related to bone density.
When the participants were divided into quartiles based on their omega-3 intake:
Participants with the highest omega-3 intake were 29% less likely to develop osteoporosis than participants with the lowest omega-3 intake.
When the investigators looked at subgroups, they found stronger effects of omega-3s on osteoporosis risk for women, people under 60, and non-smokers.
The investigators concluded, “This study demonstrates a significant inverse relationship between dietary omega-3 fatty acid intake and osteoporosis risk, suggesting omega-3s play a crucial role in bone health. This supports the need for dietary recommendations that encourage omega-3 consumption as a preventative measure against osteoporosis.”
For more information on this study, why omega-3s reduce osteoporosis risk, and what this study means for you, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
You have probably heard that moderate alcohol consumption is healthier than complete abstinence from alcohol. It is certainly a popular viewpoint.
It is also a scientific paradigm. By that I mean:
It is supported by multiple clinical studies.
Elaborate metabolic explanations have been proposed to support this paradigm.
It is the official position of most medical societies, scientific organizations, and health information sites on the web.
It is the recommendation of most health professionals.
It has been repeated so often from so many trusted sources that everyone assumes it must be true.
But is it a myth? You may have been surprised when you saw recent headlines saying, “Having an alcoholic drink or two per day is not healthier than abstaining.”
But first, I want to explain to you how the scientific method works. That’s because this study is a perfect example of the scientific method in action.
How Were We Led Astray?
I have described the scientific method in detail in my books “Slaying The Food Myths” and “Slaying The Supplement Myths”, which you will find here.
Today, I will just give you a brief synopsis of the scientific method.
1) Most scientific studies are designed to disprove existing scientific paradigms. This is such a study.
In the scientific world, there is no glory in being the 10th person to prove that a scientific paradigm is correct. The glory comes from being the first person to disprove a scientific paradigm and create a new paradigm in the process.
This constant testing of existing paradigms is one of the most important strengths of the scientific method.
2) There is no perfect study. Every study has its flaws.
“Confounding variables” are flaws that can be the Achilles Heel of any association study.
Now let me explain the significance of these statements in the context of the current study:
All the studies supporting the current paradigm were association studies. Association studies measure the association between a selected variable and an outcome. For these studies, the selected variable was alcohol consumption, and the outcome was increased mortality.
Association studies try to statistically correct for other variables known to affect the outcome. For example, diseases like heart disease, diabetes, and cancer increase the risk of premature death. These are known variables that would be corrected for in any well-designed study of alcohol consumption and mortality.
“Confounding variables” are unknown variables that also affect the outcome of the study. But since they are unknown, they are not corrected for.
Let me give you a simplistic example of a confounding variable. Let’s say you were doing a study of dietary habits, and you found an association between ice cream consumption and mortality. You might conclude that ice cream consumption is bad for you. It increases your risk of dying.
But then you might remember that ice cream consumption increases during the summer. And then you might reason that people swim more during the summer, and there is a correlation between swimming and drowning deaths.
Swimming could be a confounding variable. To make sure that your initial conclusion that ice cream increases the risk of dying was correct, you would need to correct your data for swimming deaths during the summer and see if you still found a correlation between ice cream consumption and mortality.
Could The Current Paradigm Be Incorrect?
You might be thinking, “What does this have to do with studies on the correlation between alcohol consumption and increased mortality?” Let me explain.
The baseline group for these comparisons was the abstainers – the group consuming no alcohol. Previous studies have compared the mortality risk associated with various amounts of alcohol consumption with the mortality risk of the abstainer group. This sounds like a reasonable approach.
But the investigators challenging the current paradigm noted that the “abstainer group” in previous studies included both lifetime abstainers and former drinkers who had become abstainers. They hypothesized that the “former drinkers” group may have become abstainers because of health issues related to excess alcohol consumption.
In short, they hypothesized that the “former drinkers” group was a confounding variable that biased the results of the previous studies. They hypothesized that the “lifetime abstainers” group was a more appropriate baseline group for this kind of study. They then set out to prove their hypothesis.
How Was This Study Done?
The investigators searched the literature and found 107 studies with 4.8 million participants published between 1980 and July 21, 2021, that:
Assessed the correlation between alcohol consumption and mortality.
Had data that allowed the investigators to separate lifetime abstainers from former drinkers who had become abstainers.
The investigators divided alcohol consumption into low, moderate, high, and very high categories based on the ounces of alcohol consumed per day. Since ounces of alcohol is not an easy measure for most of us, I have converted ounces/day to drinks/day based on the CDC definition of a drink (a 12-ounce beer, 5-ounce glass of wine, or 1.5 ounces of a distilled spirit like gin or vodka). And to make it even simpler, I have rounded to the nearest whole number. With that said, here are the classifications.
Low alcohol intake = 1-2 drinks/day.
Moderate alcohol intake = 2-3 drinks/day.
High alcohol intake = 3-4 drinks/day.
Very high alcohol intake = >4 drinks/day.
The risk of death associated with each of these intake levels was compared the risk of death of their preferred baseline group, the “lifetime abstainers”.
Finally, the data were corrected for other variables known to influence the correlation between alcohol consumption and mortality, namely age, sex, heart health, social status, race, diet, exercise, BMI, and smoking status. [These are known confounding variables and had been adjusted for in most previous studies.]
The Alcohol Myth
When the investigators compared the mortality risk of former drinkers who had become abstainers with lifetime abstainers:
The former drinkers were 31% more likely to die, and this difference was highly significant.
This is consistent with their hypothesis that the “former drinkers” group was a confounding variable that may have biased the conclusions of previous studies.
When they compared the mortality risk of various levels of alcohol consumption with lifetime abstainers instead of all abstainers, they found:
The risk of mortality associated with low (1-2 drinks/day) and moderate (2-3 drinks/day) alcohol intake was statistically identical to the risk of mortality for lifetime abstainers.
The high alcohol intake group (3-4 drinks/day) was 24% more likely to die than the lifetime abstainers.
The very high alcohol intake group (>4 drinks/day) was 39% more likely to die than the lifetime abstainers.
In short, when lifetime abstainers were used as the baseline group, low to moderate alcohol intake did not reduce the risk of dying, as previous studies had suggested. This study suggests the idea that low to moderate alcohol consumption is good for us may not be accurate. It may be a myth.
Finally, there was a significant gender difference in the effect of alcohol consumption on mortality.
For women:
Even moderate alcohol consumption was associated with an increased risk of mortality. Only low alcohol consumption posed no increase in mortality.
The increased risk of mortality for women was significantly higher than for men with every level of alcohol consumption.
The authors concluded, “In this…meta-analysis, daily low or moderate alcohol intake was not significantly associated with all-cause mortality risk, while increased risk was evident at higher consumption levels, starting at lower levels for women than for men.”
Of course, this isn’t the end of the story. The scientific method will continue. Old paradigms don’t die easily. Other investigators will challenge the conclusions of this study. Stay tuned. I will give you updates as future studies are published.
What Does This Study Mean For You?
If you like to imbibe, there are two important takeaways from this study.
The bad news is that you can no longer claim that a drink or two a day is healthier than total abstinence from alcohol.
The good news is that this and every study preceding it have found that a drink or two a day is no less healthy than total abstinence. The studies found no increase in mortality associated with low to moderate alcohol intake.
[However, low to moderate alcohol intake may increase your risk of specific diseases. For example, many studies suggest that even low alcohol intake is associated with an increased risk of breast cancer.]
This study also agrees with previous studies that high alcohol intake increases your risk of death, and women are more susceptible to adverse effects of alcohol intake than men.
So, while this study challenges the existing paradigm that low to moderate alcohol intake is beneficial, it does not change the current recommendations on alcohol intake by most health organizations.
For example, the current CDC guidelines are:
Adults of legal drinking age should limit alcohol intake to 2 drinks or less per day for men and one drink or less per day for women.
Adults who do not drink alcohol should not start. [The current study strengthens this recommendation because it takes away the excuse that low to moderate alcohol consumption is healthier than abstinence.]
Drinking less is better than drinking more.
The CDC guidelines also note that the risk of some cancers increases even at very low levels of alcohol consumption.
Finally, the CDC recommends that some people never consume alcohol, including:
Women who are pregnant or might become pregnant.
Anyone younger than 21.
Anyone with medical conditions or medications that interact with alcohol.
Anyone recovering from an alcohol use disorder or who has trouble controlling the amount they drink.
The Bottom Line
A recent study is a perfect example of the scientific method in action. Scientists are constantly challenging the existing scientific paradigms, and this is an important strength of the scientific method.
A group of scientists recently published a study challenging the paradigm that low to moderate alcohol intake is healthier than total abstinence from alcohol.
They hypothesized that previous studies supporting this paradigm had a common methodological flaw, corrected for the flaw, and reanalyzed the data from 104 studies with a total of 4.8 million participants.
The revised data showed no health benefit of low to moderate alcohol consumption compared to total abstinence. When you look at the data more closely, the current paradigm may be a myth.
This is a major change to the existing paradigm because it removes the justification for low to moderate alcohol consumption.
However, the revised data did not differ from previous studies in the following ways:
There is no health risk associated with low to moderate alcohol intake compared to total abstinence.
High alcohol intake (>3 drinks/day) is associated with increased mortality.
Women are more sensitive to the adverse effects of alcohol than men.
So, this study does not change current guidelines for alcohol consumption.
For more information on this study, what it means for you, and the CDC guidelines on alcohol consumption read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading Biochemistry textbooks for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
I don’t need to tell you that GLP-1 (glucagon-like peptide 1) drugs are all the rage. Total spending on GLP-1 drugs in the United States exceeded $71 billion in 2023, a 500% increase in just 5 years. There are 15 million Americans on GLP-1 drugs at any one time. And most of this increase has been driven by the weight-loss market.
Let me be clear. These drugs work. For people with poorly controlled type 2 diabetes or severe obesity-related health issues, they can be a godsend. But like any “quick fix” weight loss drug they are overprescribed.
And when you have millions of people taking a drug, you need to take a serious look at side effects. The most frequent side effects are:
Nausea
Vomiting
Diarrhea
Constipation
Increased heart rate.
Hypoglycemia
Allergic reactions
These are side effects that aren’t life threatening and are easily detected. When someone experiences these side effects, they usually give their doctor a call, and their doctor either takes them off the drug or modifies the dosage.
However, more recent studies have identified two additional side effects that are much more troubling.
The first is depression, anxiety, and suicidal thoughts.
These are symptoms that many patients may not associate with the drug, especially if they already have these tendencies.
And the consequences can be life threatening. There have already been reports of suicides of people on GLP-1 medications.
The second is loss of muscle mass.
This is a particular concern for seniors who struggle to maintain muscle mass as they age.
And this is a silent symptom. Most seniors don’t realize they are losing muscle mass until it significantly affects their quality of life.
And, of course, the biggest drawback of GLP-1 drugs is that they are only a temporary fix. Unless someone changes their lifestyle, the weight comes roaring back as soon as they quit using GLP-1.
So. It’s no wonder some people are asking whether it is possible to increase their GLP-1 levels naturally without the side effects associated with GLP-1 drugs. I will discuss this below, but first I should review what GLP-1 is and what it does.
What Is GLP-1 And What Does It Do?
Let me start by reviewing the hormones insulin and glucagon to create a proper perspective for understanding the role of GLP-1.
Insulin: Almost everyone has heard of insulin. It is released by the pancreas whenever we eat, and blood sugar levels start to rise. Its role is to lower blood sugar levels. It does this by:
Increasing glucose uptake by our cells. In the fed state almost all our cells use glucose as an energy source.
Converting any glucose in excess of immediate energy needs to storage forms.
In the muscle and liver, it is converted to a glucose polymer called glycogen. Our ability to create glycogen stores is limited.
In muscle it is also converted to amino acids, and it stimulates the use of those amino acids to make new protein. Our ability to increase muscle stores is also limited, but it can be increased by exercise.
In adipose tissue, it is converted to fat. As you may have noticed, our ability to create fat stores is unlimited. Even worse, when we become obese, fat starts accumulating in muscle and liver, which has severe health consequences.
Glucagon: Glucagon is less well known, but you can think of it as the Yin to insulin’s Yang. It is released by the pancreas when blood sugar levels fall and continues to be present until the next meal. Its role is to increase blood sugar levels and make sure that our cells get the food they need until the next meal.
Most tissues in our bodies switch to fat as an energy source in the fasting state. However, our red blood cells, kidney medulla, and brain continue to require glucose [Note: The brain can adapt to ketone bodies as an energy source after several days of glucose deprivation, but that’s another discussion for another time.] Glucagon supports our tissues by:
Signaling the liver to break down its glycogen stores and release glucose into the bloodstream. These stores are limited, but they can supply enough glucose to keep blood sugar levels constant for a few hours.
However, the brain uses lots of glucose, so the glycogen stores are rapidly depleted. When this happens, glucagon signals our muscles to break down muscle protein and convert the amino acids to glucose. We have enough muscle tissue to supply our brain with glucose for weeks. But we are using that muscle protein for other important things.
Finally, glucagon signals adipose tissue to break down its fat stores and release fat into the bloodstream to feed all our tissues that no longer depend on glucose.
GLP-1: GLP-1 stands for glucagon-like peptide 1. With a name like that, you might expect GLP-1 to have significant sequence homology with glucagon, bind to the same receptors, and have a similar effect on our metabolism. You would be wrong!
Both peptide hormones are derived from a much larger peptide called proglucagon. This is the only way that GLP-1 is “like” glucagon.
One portion of proglucagon is processed to give glucagon in pancreatic alpha cells. Another portion is processed to give GLP-1 in intestinal L cells. [L cells are endocrine (hormone producing cells) found in the intestinal mucosa.] There is very little sequence or structural homology between glucagon and GLP-1.
Their function is also very different. You can think of GLP-1 as a partner to insulin. It is released by intestinal L cells in response to the presence of nutrients (primarily protein, fat, and carbohydrate) in the intestine. It binds to GLP-1 receptors on the…
Pancreas to stimulate insulin release and inhibit glucagon release. This is why it helps type 2 diabetics control their blood sugar levels.
Stomach and reduces the rate of gastric emptying. This prolongs the feeling of fullness after each meal.
Small intestine and reduces gut motility, which increases transit time through the small intestine. This prolongs the feeling of fullness after a meal. But it can also lead to gastrointestinal side effects.
Brain and turns down your “appestat”. This reduces feelings of hunger between meals. But at high doses, it can affect the brain in negative ways (anxiety, depression, and suicidal thoughts).
Increasing GLP-1 Levels Naturally
At the beginning of this article, I asked the question, “Is it possible to increase GLP-1 levels naturally without side effects?” The answer is clearly, “Yes”. Every time you eat a meal, your GLP-1 levels increase naturally.
GLP-1 levels rise within 10 minutes after consuming a meal and remain elevated for 1-2 hours. Then enzymes present in the bloodstream digest GLP-1 and it disappears. This is the way nature intended. There are no side effects to the natural rise and fall of GLP-1 after a meal.
“What makes the GLP-1 drugs different?”, you might ask.
In the first place significantly higher doses of GLP-1 are used.
More importantly, GLP-1 drugs have been genetically modified to make them resistant to enzymatic digestion. They can stay in the bloodstream for up to 24 hours.
This is what makes them so effective as weight loss drugs. But it’s not nice to fool with mother nature. This is also why they have side effects.
What Does This Mean For You?
Let’s start by remembering that while GLP-1 drugs are effective, you will need to take them for the rest of your life unless you change your diet and lifestyle. And with long-term usage of the drugs, you are likely to experience one or more of their side effects at some point.
So, if you are willing to change your diet and lifestyle, it may be worthwhile looking at increasing your GLP-1 levels naturally. You have lots of options.
Every time you eat a meal your GLP-1 levels increase. And the bigger the meal, the bigger the increase. But the bigger the meal, the greater the calories. So, that’s not an optimal way to increase GLP-1 levels.
The macronutrients fat, carbohydrate, and protein all increase GLP-1 levels.
But if you are trying to lose weight, you want the greatest increase in GLP-1 with the fewest calories. That leaves out fatty foods.
You could try high carbohydrate meals, but there are lots of reasons why that’s not a good choice.
That leaves protein. And since you are trying to maximize GLP-1 levels with the minimum calories, I recommend a 20–40-gram protein supplement with a minimum of carbohydrate and fat. Just be sure the manufacturer has done a clinical study to demonstrate their protein supplement raises GLP-1 levels.
The Bottom Line
In this article I asked the question, “Is it possible to increase GLP-1 levels naturally without the side effects of GLP-1 drugs?” The answer is, “Yes”. In this article I tell you:
What GLP-1 is and what it does.
Why GLP-1 drugs have side effects.
How to raise your GLP-1 levels naturally without the side effects of GLP-1 drugs.
For more details read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
Most people want to lose weight so they can get trimmer and healthier. I don’t know of anyone who wants to be leaner and less healthy. But if they are not getting the essential nutrients their body needs while they are losing weight, they may well end up both lean and unhealthy.
I don’t need to tell you that GLP-1 (glucagon-like peptide 1) drugs are all the rage. Total spending on GLP-1 drugs in the United States exceeded $71 billion in 2023, a 500% increase in just 5 years. There are 15 million Americans on GLP-1 drugs at any one time. And most of this increase has been driven by the weight-loss market.
GLP-1 drugs do work. They target the intestine and the brain, increasing satiety (feeling of fullness) and decreasing appetite.
However, like any other drug, they have side effects. The most frequent are:
Nausea
Vomiting
Diarrhea
Constipation
Increased heart rate.
Hypoglycemia
Allergic reactions
In a previous issue of “Health Tips From the Professor” I discussed a serious side effect that is often overlooked, namely increased risk of depression, anxiety, and suicidal thoughts. My recommendations were:
If you suffer from depression, anxiety, or suicidal thoughts, GLP-1 drugs may not be the best choice for you. At the very least you should discuss the risks and benefits with your doctor before using them.
If you are using GLP-1 drugs and experience an increase in depression, anxiety, or suicidal tendencies, you should discontinue the drug immediately and report your side effects to your doctor.
Another question that has not been addressed previously is whether people using GLP-1 drugs are getting the essential nutrients their bodies need for optimal health. Today’s study (B Johnson et al, Frontiers in Nutrition, published online in April 2025) was designed to measure the nutritional adequacy of GLP-1 user’s diets.
How Was This Study Done?
The investigators enrolled 69 people who had been using a GLP-1 drug for at least a month in their study using an online research platform through the University of Turin in Italy.
The characteristics of the study participants were:
Weight:
5% normal weight
27% overweight
18% Obese Class I
20% Obese Class II
30% Morbidly Obese
Age = 49.6 ± 12.3
Ethnicity:
82% Caucasian
6% Hispanic
8% African American
1% Asian
This is similar to the ethnic distribution of GLP-1 users in this region.
Length of GLP-1 use:
7% <3 months
29% 4-6 months
25% 7-12 months
39% >1 year
The participants were trained on how to use an online dietary recall instrument and then recorded their dietary intake for 3 consecutive days.
Are GLP-1 Users Getting Enough Nutrients?
The results of the 3-day dietary recalls from the GLP-1 users were:
Their diets were high in fat (39% of calories) and saturated fat (13%).
Their diets were low in fruit, vegetables, grains, and dairy foods.
Their diets were low in fiber (14 grams). This is half the recommended intake of fiber.
Their diets were sufficient for B-vitamins, copper, phosphorous, selenium, and zinc.
Their diets were deficient for calcium, iron, magnesium, potassium, choline, vitamin A, vitamin C, vitamin K, vitamin D, vitamin E, and fiber. For example:
99% of participants were not getting enough Vitamins D and K from their diet.
94% weren’t getting enough choline.
90% weren’t getting enough magnesium.
88% weren’t getting enough iron.
The study did not report the intake of omega-3 fats, but the participants were likely deficient in that as well.
The study participants averaged 0.8 gm/kg of protein, which is the recommended intake for sedentary adults who are not on a weight loss diet. However, 0.8 gm/kg of protein is not sufficient for maintaining muscle mass on weight loss diets, especially weight loss diets aided by GLP-1 drugs. Most experts recommend 1.2gm/kg to 1.6 gm/kg to prevent loss of muscle mass, with a few recommending as high as 2 gm/kg.
Most of the participants in this study did not meet the increased protein recommendations for weight loss.
Only 43% consumed at least 1.2 gm/kg of protein.
Only 10% consumed at least 1.6 gm/kg of protein.
Only 5% consumed at least 2.0 gm/kg of protein.
The authors concluded, “Participants on a GLP-1 drug are not meeting the DRI [daily recommended intake] for several vital nutrients through their diet or the higher protein needs during weight loss. Patient-centered nutritional guidance is essential to optimize health outcomes and prevent unintended health consequences.
What Does This Mean For Your Future Health?
The results of this study are both appalling and expected. Weight loss diets often result in nutritional insufficiencies. However, GLP-1-aided weight loss is worse.
That’s because GLP-1 is a drug, not a diet plan. It’s dispensed like any other drug.
Your doctor gives you a GLP-1 prescription. If you are lucky, they may give you a “one-size-fits-all” handout on how to lose weight while you are using it. For example, in this study:
Only 51% of participants received information from their doctor on how to manage side effects of GLP-1.
Only 20% were referred to a dietitian. The other 80% received no information on how to change their diet and lifestyle.
When you pick up the drug from the pharmacy, you get a package insert listing the side effects but no information on how to change your diet.
The results were predictable:
From a medical point of view the results were a big success:
The participants in the study reduced their caloric intake by 20%.
Most of the participants in the study felt the GLP-1 drug was helping them lose weight.
But from a nutritional point of view the study raises a red flag. Most of the participants were not told to change their diet or lifestyle, and they didn’t. Their diet was still:
High in total fat and saturated fat and probably low in healthy fats, although that was not assessed.
Low in fruits, vegetables, grain, dairy, and fiber.
The typical American diet is bad enough as it is. But when you eat the same diet and decrease calories, the nutritional inadequacies of the American diet are magnified. That is why the diets of the GLP-1 users were deficient in fiber plus 10 essential vitamins and minerals and did not contain enough protein to prevent loss of muscle mass.
Most (52%) of the participants were planning to be on GLP-1 drugs for a short period of time – just long enough to reach their weight loss goals. But the reality is far different.
Studies show that when people lose weight on GLP-1 drugs without changing their diet and lifestyle, the weight comes roaring back as soon as they get off the drugs. The reality is that those people will need to stay on GLP-1 drugs for a lifetime if they want to keep the weight off.
That’s when the nutritional inadequacies shown in this study start to have real health consequences. For example,
Long term inadequacies of calcium, magnesium, and vitamin D increase the risk of osteoporosis.
Long term muscle loss due to inadequate protein intake leads to frailty and metabolic diseases as we age.
I could go on, but you get the point. GLP-1 drugs are not a panacea. Without diet and lifestyle change, they are just a temporary and expensive solution to weight loss.
The Bottom Line
A recent study looked at the nutritional intake of GLP-1 users. It found:
Their diets were high in fat (39% of calories) and saturated fat (13%).
Their diets were low in fruit, vegetables, grains, and dairy foods.They were deficient in fiber plus 10 essential vitamins and minerals.
They were not getting enough protein to prevent the loss of muscle mass associated with GLP-1 use for weight loss.
The authors concluded, “Participants on a GLP-1 drug are not meeting the DRI [recommended intake] for several vital nutrients through their diet or the higher protein needs during weight loss. Patient-centered nutritional guidance is essential to optimize health outcomes and prevent unintended health consequences.
For details about the study and the health consequences of these nutrient deficiencies, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”.
Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
How do the myths of the food supplement industry originate? Some of them start innocently enough. They are often based on a kernel of truth which is misinterpreted by some well-meaning medical doctors.
It’s not their fault. We teach future doctors what I call “metabolism light” in medical school. There simply isn’t room in the medical curriculum to teach all the details and nuances of human metabolism.
We also try to teach them the basics of how to interpret scientific literature. However, it takes years of experience to get good at picking out the strengths and weaknesses of clinical studies.
The doctors form their hypothesis and test it on a few patients. If it works, they publish a paper. At that point their idea is picked up by the “sensationalist” bloggers. These are the bloggers who like to focus on the sensational. They delight in writing about “new findings” that go against what the medical profession has been telling you for years.
The bloggers don’t stop there. They usually expand the claims. They ‘cherry pick” the scientific literature by quoting only studies that support their viewpoint and ignoring studies that refute it. In short, they put together a very compelling story. Soon the story is picked up by other bloggers who embellish it further. After it appears in enough sites, people start believing it. A myth is born.
Then supplement companies get in the act. They sense there is money to be made. They manufacture supplements to provide nutrients supported by the myths. They embellish the mythology even more and put together a compelling story to market their products.
This is where the mythology becomes deception. Companies have the responsibility to design their products based on the best science. They have an obligation to tell the truth about their products. When they make claims they know cannot be true, they are lying to you.
The saga of methylfolate is a perfect example of how observations based on a kernel of truth became myths and eventually became downright lies. Let me share that story with you.
The Kernel Of Truth About Methylfolate
Let’s start with one of the “kernel of truth” that launched the whole methyl folate saga. It started with a doctor who was having a very difficult time finding a solution for a patient with some significant health issues. The doctor ordered a genetic test and discovered the patient had a deficiency in the methylene tetrahydrofolate reductase (MTHFR) gene.
The doctor remembered the reaction catalyzed by MTHFR, and a light bulb went off. “Eureka”, he said. His patient must be unable to make N5-methyltetrahydrofolate (commonly referred to as methylfolate or methyl folate), and methylfolate is required for some very important methylation reactions in the cell.
He gave his patient methylfolate, and the patient’s symptoms got better. The doctor leapt to the conclusion that other patients with MTHFR deficiency needed methylfolate as well. Many of those patients responded to methylfolate as well. He didn’t bother to check whether they responded equally well to folic acid. He just assumed methylfolate was the magic elixir.
He wrote a paper on his clinical observations, and the methylfolate story was launched. It all seemed so logical.
However, the story was not nearly as straight forward as the doctor and the people publicizing his findings assumed. Let me walk you through some “Metabolism 101”. Don’t worry. There won’t be a quiz.
Why The Original Assumptions About Methylfolate Were Misleading
MTHFR mutants only have a partial loss of activity.
Individuals with 2 copies of a mutation from A to C at position 1298 of the MTHFR gene (A1298C homozygotes) comprise about 5% of the US population. They have 60% enzyme activity and appear to be normal in clinical studies.
Individuals with 2 copies of a mutation from C to T at position 677 of the MTHFR gene (C677T homozygotes) have 30% enzyme activity. They comprise about 10% of the US population. C677T homozygotes often have elevated homocysteine levels. The homozygous C677T mutation is associated with depression, anxiety, and mood swings in some people, but not in others (I will come back to the significance of that qualifying statement later).
C677T heterozygotes (one mutant gene) have 65% activity and are normal.
We Don’t Need 100% MTHFR Activity
Our human body is wonderfully designed. For many of our most essential metabolic reactions we have built in redundancy. We don’t require 100% activity of key enzymes. This helps protect us from bad effects of mutations as they arise.
The best analogy I can think of is the US space program. Most space vehicles had built in redundancy so that if one system failed, the mission could go on. For example, you may remember the Hubble space telescope. It was launched with four gyroscopes to keep the telescope pointed in the right direction.After a few years, one gyroscope gave out. That was not a problem because there were three left. A few years later the second gyroscope gave out. Again, there was no problem because there were still two gyroscopes left.
It was only after the third gyroscope gave out that Hubble became a bit “wonky”, and a space shuttle was sent up to replace the gyroscopes. It is the same with MTHFR. Only when you get down to around 30% activity, does it become a bit wonky”. (That’s about as non-technical as I get.)
Not Everyone With MTHFR Deficiency Experiences Symptoms
This is due to a phenomenon my geneticist friends refer to as penetrance. Simply put, that means that not everyone with the same mutation experiences the same severity of symptoms. That is because the severity of a mutation is influenced by diet, lifestyle, and genetic background.
Let me start with genetic background. In terms of MTHFR mutants you can think of genetic background as being mutations in a related methylation pathway. People who have a mutation in both MTHFR and a gene in a related pathway will experience more severe symptoms and are more likely to require methylfolate. Once you understand penetrance, you realize that individuals requiring methylfolate may represent only a small subset of people with MTHFR mutations.
Penetrance is a concept that most proponents of the methylfolate hypothesis completely ignore. The most severe MTHFR mutation (C677T homozygote) increases the probability that individuals will exhibit symptoms, but some individuals with that mutation are completely normal. Now that you understand the concepts of redundancy and penetrance, you can understand why that is.
When Did The Kernel of Truth Become A Myth?
Up to this point the hype around methylfolate could be chalked up to an honest misunderstanding.
The doctors who published the original papers may not have known that MTHFR mutations only resulted in a partial reduction in enzyme activity.
They probably didn’t know the concepts of redundancy (our cells don’t need 100% enzyme activity) or penetrance (the same mutation may cause severe symptoms in some patients and have no effect in others).
It seemed logical to assume that everyone with a MTHFR mutation might do better with methylfolate supplementation. That was incorrect, but it was an honest mistake.
However, the message was picked up by the bloggers who specialize in sensational stories, especially stories that contradict what experts have been telling you for years. They picked up the methylfolate story and distorted it beyond recognition.
They knew that “natural” is a buzz word, so they told you that methylfolate was natural and folic acid is synthetic.
They told you that methylfolate was better utilized than folic acid.
They told you that methylfolate was more effective than folic acid.
They told you folic acid was toxic. It was going to increase your risk of cancer.
Suddenly, it was no longer about people with MTHFR deficiency. You were told that everyone should avoid folic acid and use methylfolate instead.
On the surface, these pronouncements should not have passed the “If it sounds too good to be true…” test, or in this case, the “If it sounds too bad to be true…” test. You were being asked to believe that folic acid, which has been in use for over 80 years and is backed by hundreds of studies showing it is safe and effective, was neither safe nor effective. You were asked to believe that the government was poisoning you by fortifying foods with folic acid.
However, to make their blogs sound more convincing, they listed clinical studies supporting their stories. The problem is they “cherry picked” the studies that supported their story and ignored the rest. Their bias was particularly outrageous when it came to the “story” that folic acid increases cancer risks. They ignored 10 or 20 studies showing no cancer risk and reported one suggesting it might increase risk. I call that deceptive.
Unfortunately, the myths created by the bloggers have been repeated often enough that many people now believe they are true. It is time for me to debunk the methylfolate myths.
The Methylfolate Myths
Myth: Methylfolate is natural. It comes from whole food. Folic acid is synthetic.
Fact: Methylfolate is chemically synthesized from folic acid. It is physically impossible to extract enough from whole foods. Here are the facts:
Methyfolate is only one of several naturally occurring folates in foods.
The best food sources of folates are beans, leafy greens, and broccoli.
To obtain the RDA of methyfolate for a single tablet you would need to start with 1 cup of lentils, two cups of cooked spinach, or 4 cups of broccoli.
You do the math! It just isn’t possible.
Myth: Methylfolate is better utilized by the body than folic acid.
Fact: This claim is based on levels of methylfolate in the blood after taking supplements providing equivalent amounts of methylfolate and folic acid. However, methylfolate has no biological activity in our blood. The measurement that matters is total folate levels (methylfolate plus other folates) in our cells.
If you take equivalent amounts of folic acid and methylfolate, you end up with identical folate levels in your cells (B.J. Venn et al, The Journal of Nutrition, 132: 3333-3335, 2002) In short, there is no difference in our ability to utilize methylfolate and folic acid.
Myth: If you have a mutation in the MTHFR gene, folic acid isn’t effective.
Fact: MTHFR slightly increases the need for folic acid (from 400 ug to between 600 and 800 ug), but multiple studies show that folic acid supplementation is effective in people with MTHFR mutations.
For example, homocysteine levels are easily measured and are a reliable indicator of methylfolate status.
One study has shown that folic acid and methylfolate were equally effective at lowering plasma homocysteine in people who were MTHFR C677T homozygotes (P. Fohr et al, American Journal of Clinical Nutrition, 75: 275-282, 2002).
That study also showed that folic acid was more effective than methylfolate at lowering homocysteine in people who were C677T heterozygotes and in people with normal MTHFR activity.
Another study showed folic acid was just as effective as a diet providing equivalent quantities of folate from foods at lowering homocysteine levels in people with various MTHFR mutations (A. Ashfield-Watt et al, American Journal of Clinical Nutrition, 76: 180-186, 2002).
At present, lowering of homocysteine levels is the only indicator of methylfolate status for which methylfolate and folic acid have been directly compared. However, there are other studies suggesting that folic acid is likely to be effective for people with MTHFR defects. For example:
Folic acid has been shown in multiple studies to be effective in preventing neural tube defects (M. De-Regil et al, Cochrane Database Systematic Reviews 2010 Oct 6;(10):CD007950. PMID: 20927767), which are highly associated with the C677T MTHFR gene defect.
Three studies have shown that supplementation with folic acid, B12, and B6 slowed cognitive decline in older people with elevated homocysteine levels ( Durga et al, The Lancet, 369: 208-216, 2007; A.D. Smith et al, PLoS ONE 5(9): e12244. doi:10.1371/journal.pone.0012244, 2010; G. Douaud et al, Proceedings of the National Academies of Sciences, 110: 9523-9528, 2013).
In contrast, the one study that substituted methylfolate for folic acid showed no effect (A. McMahon et al, New England Journal of Medicine, 354: 2764-2769, 2006).
Myth: Folic acid causes cancer.
Fact:The few studies suggesting that folic acid supplementation might increase the risk of cancer were “outliers”. By that I mean they contradicted many other studies showing no increased risk.
Scientists are accustomed to this. We know that studies sometimes come up with conflicting results. In some cases, we can point to an error in experimental design or statistical analysis as the cause of the aberrant results.
In other cases, we never know the reason for the differences, so we go with the weight of experimental evidence (what the majority of studies show). The weight of evidence clearly supports the safety of folic acid,
However, that is not enough. If there is the slightest possibility that something causes cancer, we investigate it further. Consequently, the scientific community followed up with larger studies.
Those studies showed either reduced cancer risk or no difference in cancer risk with folic acid supplementation. None of the studies found any evidence that folic acid increased cancer risk. I have covered this in detail for folic acid and colon cancer risk in a previous issue of “Health Tips From The Professor”.
There have also been a couple of small studies suggesting that folic acid might increase the risk of prostate and breast cancer. Although these were small, individual studies, they have been widely hyped by the methylfolate advocates. Once again, the definitive study has been done (S.E. Vollset et al, The Lancet, 381: 1029-1036, 2013).
It was a meta-analysis of 13 placebo-controlled studies involving over 50,000 subjects. The results were clear cut. Folic acid supplementation caused no increase in overall cancer risk, and no increase in the risk of colon cancer, prostate cancer, breast cancer, or any other individual cancer. Moreover, the average dose of folic acid in those studies was 2 mg/day, which is 5 times the RDA.
Of course, the bloggers and the companies selling methylfolate supplements ignore the definitive studies showing folic acid does not increase cancer risk. The myths and lies continue.
Myth: Folic acid can mask a B12 deficiency.
Fact: True but irrelevant if you use a supplement with folic acid and B12 in balance.
The Lies Of The Supplement Industry
If you are writing a blog, you are covered by “freedom of speech”. You can say whatever you want. It doesn’t have to be true. However, if you are a supplement manufacturer, you are held to a higher standard. Ignorance is no longer an excuse. You can no longer cherry pick the “facts” you like and ignore the rest. You are ethically obligated to research all the available literature and be guided by the best scientific evidence.
Reputable companies have been guided by scientific evidence and have not jumped on the methylfolate bandwagon. They know folic acid is both safe and effective in a wide variety of clinical situations. They also know that, while methylfolate may be just as effective as folic acid, it has not been shown to be superior to folic acid for any clinical application.
They may offer a methylfolate option for people who believe they need it. But they make no claim that it is superior to their products containing folic acid.
Less reputable companies, however, sensed money to be made by capitalizing on the buzz around methylfolate. They repeated the myths of the bloggers and claimed their products were superior to others on the market. They call it marketing. I call it lying. They have an obligation to fact check their claims and only make claims that are true.
Let me give you an example. In preparing for this article, I looked at the claims of several companies that were promoting their methylfolate supplements. One in particular claimed they had studies showing:
Their methylfolate supplement was effective at reducing the risk of adverse pregnancy outcomes.
Their methylfolate supplement was twice as bioavailable as folic acid.
Their methylfolate supplement was able to lower homocysteine levels better than conventional folic acid supplementation.
All three studies were bogus.
With respect to the first study, it was likely true that their methylfolate supplement decreased adverse pregnancy outcomes. But there are dozens of studies showing that folic acid does the same thing.
And because they did not compare methylfolate and folic acid supplementation in their studies, they have no basis for claiming their supplement was superior.
The second study compared levels of methylfolate and folic acid in the blood. As I mentioned above, methylfolate has no biological activity in our blood. The measurement that matters is total folate levels (methylfolate plus other folates) in our cells. And previous studies have shown that equivalent amounts of methylfolate and folic acid give identical amounts of methyfolate in our cells.
The third study compared their supplement, which contained B6, B12, zinc, and betaine in addition to methylfolate, to folic acid alone. That’s comparing apples to oranges. That is because there are three pathways for lowering homocysteine levels, and B6, B12, and betaine play important roles in each of these pathways.
B12 is an integral part of the enzyme methionine synthase, an enzyme that converts homocysteine to the amino acid methionine. Methylfolate transfers its methyl group to the enzyme-bound vitamin B12, and methyl B12 transfers the methyl group to homocysteine, which converts it to methionine. In other words, methylfolate cannot lower homocysteine levels by itself. It needs vitamin B12.
Betaine also serves as a methyl donor in another pathway for converting homocysteine to methionine by an enzyme called betaine-homocysteine methyltransferase.
B6 is essential for yet another pathway that lowers homocysteine levels by converting homocysteine to the amino acid cysteine.
You might argue that the company was simply ignorant of the importance of B6, B12, and betaine for lowering homocysteine levels. However, that is unlikely. Why else would they have included B6, B12, and betaine in their supplement?
They must have known the study they designed was bogus. That suggests they conducted the study with the sole purpose of deceiving you, the consumer. I call that lying.
Finally, in case you were wondering, I am not recommending you select a single supplement with folic acid, B6, and B12. I do recommend you get your folic acid from a multivitamin or B complex supplement that provides all three B vitamins in balance.
Betaine deficiency is very rare, so I don’t include betaine in my recommendations.
What Does This Mean For You?
MTHFR mutations only result in partial loss of activity. Most individuals with MTHFR defects remain symptom free with the RDA, or slightly above the RDA, of folic acid.
However, there may be some individuals with a MTHFR defect and additional gene defects in metabolic pathways involving methylation who might benefit from methylfolate. This is due to a phenomenon that geneticists call penetrance and would likely represent a small subset of the population with MTHFR defects.
Finally,the claims that everyone would benefit from methylfolate instead of folic acid are false. They are contradicted by human metabolism and multiple published clinical studies.
In short, folic acid has been used for over 80 years. There are hundreds of clinical studies showing it is safe and effective, even in most individuals with a MTHFR deficiency. I can’t tell you whether the companies selling methylfolate are ignorant of basic metabolism and the published studies refuting their claims or whether they are purposely trying to deceive the public—but neither is a good thing.
The Bottom Line
Some supplement manufacturers are claiming that methylfolate is more natural and more effective than the folic acid that has been used in supplements for the past 80 years. In this issue of “Health Tips From the Professor” I debunk the methylfolate myths used by the supplement manufacturers to sell their methylfolate products.
I can’t tell you whether the companies selling methylfolate are ignorant of basic metabolism and the published studies refuting their claims or whether they are purposely trying to deceive the public—but neither is a good thing.
For more specifics, read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry textbooks for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 53 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.
 Cold and flu season is here. And if you have children, that’s not good news. Children and adolescents are particularly susceptible to respiratory infections (colds, sore throat, sinusitis, pneumonia, and bronchitis). That’s because:
Cold and flu season is here. And if you have children, that’s not good news. Children and adolescents are particularly susceptible to respiratory infections (colds, sore throat, sinusitis, pneumonia, and bronchitis). That’s because: The authors of this study used data from the 2017-2018 National Health and Nutrition Examination Survey (NHANES) in the United States. The NHANES study included 8,704 people, of which 1,344 were children or adolescents aged 6-19 years old.
The authors of this study used data from the 2017-2018 National Health and Nutrition Examination Survey (NHANES) in the United States. The NHANES study included 8,704 people, of which 1,344 were children or adolescents aged 6-19 years old. The results were clear cut:
The results were clear cut: This study suggests that vitamin C supplementation may help protect our children and grandchildren from respiratory infections. However, we need to acknowledge the strengths and limitations of the study.
This study suggests that vitamin C supplementation may help protect our children and grandchildren from respiratory infections. However, we need to acknowledge the strengths and limitations of the study.
 Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years.