Can Chocolate Help You Lose Weight?
Author: Dr. Stephen Chaney
 Sometimes you come across news that just seems too good to be true. The claims that you can lose weight just by eating chocolate are a perfect example. Your first reaction when you heard that was probably “Sure, when pigs fly!”
Sometimes you come across news that just seems too good to be true. The claims that you can lose weight just by eating chocolate are a perfect example. Your first reaction when you heard that was probably “Sure, when pigs fly!”
But it’s such an enticing idea – one might even say a deliciously enticing idea. And, in today’s world enticing ideas like this quickly gain a life of their own. Two popular books have been written on the subject.
Chocolate diet plans are springing up right and left. A quick scan of the internet even revealed a web site saying that by investing a mere $1,250 in a training course you could become a “Certified Chocolate Weight Loss Coach” earning $50,000/year.
If you like chocolate as much as most people you are probably wondering, “Could it possibly be true, or is it just another myth?
Can Chocolate Help You Lose Weight?
 The idea that chocolate could help you lose weight does have some support. There are actually three published clinical studies suggesting that chocolate consumption is associated with lower weight (European Journal of Clinical Nutrition, 62: 247-253, 2008; Nutrition Research, 31: 122-130, 2011; Archives of Internal Medicine, 172: 519-521, 2012).
The idea that chocolate could help you lose weight does have some support. There are actually three published clinical studies suggesting that chocolate consumption is associated with lower weight (European Journal of Clinical Nutrition, 62: 247-253, 2008; Nutrition Research, 31: 122-130, 2011; Archives of Internal Medicine, 172: 519-521, 2012).
While that sounds impressive, they were all cross-sectional studies. That means they looked at a cross section of the population and compared chocolate intake with BMI (a measure of obesity). Cross sectional studies have a couple of very important limitations:
1) Cross sectional studies merely measure associations. They don’t prove cause and effect. Was it chocolate that caused the lower weight, or was it something else that those populations were doing? We don’t really know.
2) Cross sectional studies don’t tell us why an association occurs. In many ways, this is the old chicken and egg conundrum. Which comes first? In this case the question is whether the people in the studies became obese because they ate less chocolate – or did they eat less chocolate because they were obese and were trying to control their calories? Again, we have no way of knowing.
The Chocolate Myth
 Chocolate is relatively rich in fat and high in calories. It’s not your typical diet food. On the surface, it seems implausible that eating chocolate could actually help you lose weight.
Chocolate is relatively rich in fat and high in calories. It’s not your typical diet food. On the surface, it seems implausible that eating chocolate could actually help you lose weight.
Scientists love to poke holes in implausible hypotheses, so it is no surprise that a recent study (JA Greenberg and B Buijsse, PLOS ONE, 8(8) e70271) has poked some huge holes in the “chocolate causes weight loss” hypothesis.
This study analyzed data from over 12,000 participants in the Atherosclerosis Risk in Community (ARIC) Study. This was also a cross-sectional study, but it was a prospective, cross-sectional study (That’s just a fancy scientific term which means that the study followed a cross section of the population over time, rather than just asking what that population group looked like at a single time point).
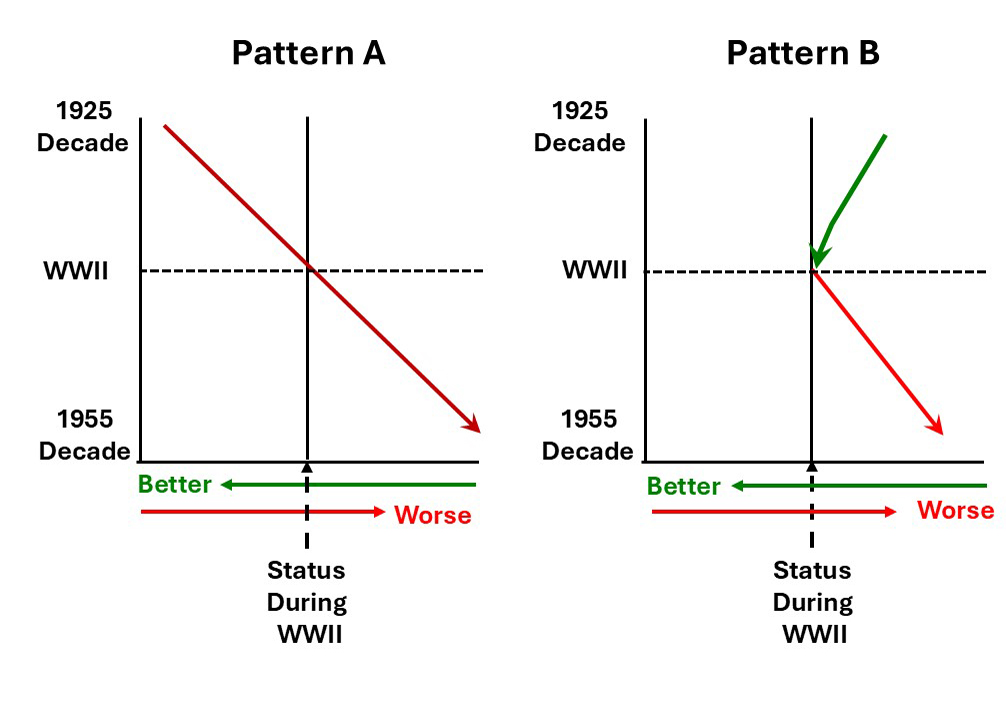
The authors of the study assessed frequency of chocolate intake and weight for each individual in the study at two separate times 6 years apart. The results were very interesting:
- When they looked at a cross section of the population at either time point, their results were the same as the previous three studies – namely those who consumed the most chocolate weighed less. So, the cross-sectional data were consistent. Overweight people consumed less chocolate. But that still doesn’t tell us why they consumed less chocolate.
- However, when they followed the individuals in the study over 6 years, those who consumed the most chocolate gained the most weight. The chocolate eaters were skinnier than the non-chocolate eaters at the beginning of the study, but they gained more weight as the study progressed. And the more chocolate they consumed the more weight they gained over the next 6 years. [No surprise here. Calories still count.]
- When they specifically looked at the population who had developed an obesity-related illness between the first and second time point, they found that by the end of the study those participants had:
-
- Decreased chocolate intake by 37%
- Decreased fat intake by 4.5%
- Increased fruit intake by 20%
- Increased vegetable intake by 17%
- In short, this study is more consistent with the “obesity causes reduced chocolate intake” model than the “reduced chocolate intake causes obesity” model. Simply put, if you are trying to lose weight, sweets like chocolate are probably among the first things to go.
Of course, even prospective cross-sectional studies have their limitations. Double blind, placebo-controlled studies are clearly needed to resolve this question. The only published study of this type has reported a slight weight gain associated with 25 g/day of dark chocolate, but the study was too small and too short in duration to draw firm conclusions.
In summary, more studies are needed, but the current evidence does not support the “miracle diet food” claims for chocolate. This appears to be another food myth. Pigs are flying!
The Bottom Line:
- Pigs still haven’t learned how to fly. As enticing as it may sound, the weight of current evidence does not support the claims that chocolate is a miracle diet food or that eating chocolate every day is a sensible strategy for losing weight.
- On the other hand, dark chocolate is probably one of the healthier dessert foods. There is no reason not to enjoy an occasional bite of chocolate as part of a healthy, calorie-controlled diet.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
_____________________________________________________________________________
My posts and “Health Tips From the Professor” articles carefully avoid claims about any brand of supplement or manufacturer of supplements. However, I am often asked by representatives of supplement companies if they can share them with their customers.
My answer is, “Yes, as long as you share only the article without any additions or alterations. In particular, you should avoid adding any mention of your company or your company’s products. If you were to do that, you could be making what the FTC and FDA consider a “misleading health claim” that could result in legal action against you and the company you represent.
For more detail about FTC regulations for health claims, see this link.
https://www.ftc.gov/business-guidance/resources/health-products-compliance-guidance
_______________________________________________________________________
About The Author
Dr. Chaney has a BS in Chemistry from Duke University and a PhD in Biochemistry from UCLA. He is Professor Emeritus from the University of North Carolina where he taught biochemistry and nutrition to medical and dental students for 40 years. Dr. Chaney won numerous teaching awards at UNC, including the Academy of Educators “Excellence in Teaching Lifetime Achievement Award”. Dr Chaney also ran an active cancer research program at UNC and published over 100 scientific articles and reviews in peer-reviewed scientific journals. In addition, he authored two chapters on nutrition in one of the leading biochemistry text books for medical students.
Since retiring from the University of North Carolina, he has been writing a weekly health blog called “Health Tips From the Professor”. He has also written two best-selling books, “Slaying the Food Myths” and “Slaying the Supplement Myths”. And most recently he has created an online lifestyle change course, “Create Your Personal Health Zone”. For more information visit https://chaneyhealth.com.
For the past 45 years Dr. Chaney and his wife Suzanne have been helping people improve their health holistically through a combination of good diet, exercise, weight control and appropriate supplementation.