Creating A “Bone Healthy” Lifestyle
Author: Dr. Stephen Chaney
 A recent study (Tai et al, British Medical Journal, BMJ/2015; 351:h4183 doi: 10.1136/bmj.h4183)reported that calcium supplementation for women over 50 resulted in only a very small increase in bone density, which translated into a very small (5-10%) decrease in the risk of bone fractures. They concluded that the standard RDA recommendation of 1,000 – 1,200 mg/day of calcium for adults over 50 is unlikely to help in preventing osteoporosis or reducing the risk of bone fractures.
A recent study (Tai et al, British Medical Journal, BMJ/2015; 351:h4183 doi: 10.1136/bmj.h4183)reported that calcium supplementation for women over 50 resulted in only a very small increase in bone density, which translated into a very small (5-10%) decrease in the risk of bone fractures. They concluded that the standard RDA recommendation of 1,000 – 1,200 mg/day of calcium for adults over 50 is unlikely to help in preventing osteoporosis or reducing the risk of bone fractures.
In last week’s issue of “Health Tips From the Professor,” I discussed the many flaws of the study. In brief:
- The study was a meta-analysis of 51 published clinical studies. Normally, meta-analyses are very strong, but they have an “Achilles Heel” – something called the Garbage-In, Garbage-Out Simply put, this means that the meta-analysis is only as strong as the individual studies that went into it. The authors included 40 years of clinical studies in their meta-analysis, and most of those studies had an inadequate design by today’s standards.
- The study also made a number of what I would call apples to oranges comparisons that were of questionable validity.
In this week’s issue of “Health Tips From The Professor”, I would like to explore the other side of the coin. I would like to consider the possibility that the study might be correct and discuss what that might mean for you.
What Is A “Bone Healthy” Lifestyle?
Despite the concerns I just mentioned, let’s assume for a minute that the study might just be correct in spite of its many flaws. Let’s assume that the “one size fits all” RDA recommendation of 1,000 – 1,200 mg/day of calcium if you are over 50 may actually be flawed advice. If so, perhaps it’s time to say good riddance! It may finally be time to put away the “magic bullet”, “one size fits all” thinking and start seriously considering holistic approaches.
Now that I have your attention, let’s talk about what you can do to prevent osteoporosis – and the role that supplementation should play. Let’s talk about a “bone healthy” lifestyle.
#1: Let’s start with supplementation: Bone is not built with calcium alone. Bone contains significant amounts of magnesium along with the trace minerals zinc, copper and manganese – and all of these are often present at inadequate levels in the diet. Most of us know by now that vitamin D is essential for bone formation, but recent research has shown that vitamin K is also essential (Kanellakis et al, Calcified Tissue International, 90: 251-262, 2012). An ideal calcium supplement should contain all of those nutrients.
 #2: Next comes diet: Many of you probably already know that some foods are acid-forming and other are alkaline-forming in our bodies – and that it is best to keep our bodies on the alkaline side. What most of you probably don’t know is that calcium is alkaline and that our bones serve as a giant buffer system to help keep our bodies alkaline. Every time we eat acid-forming foods a little bit of bone is dissolved so that calcium can be released into the bloodstream to neutralize the acid. (My apologies to any chemists reading this for my gross simplification of a complex biological system).
#2: Next comes diet: Many of you probably already know that some foods are acid-forming and other are alkaline-forming in our bodies – and that it is best to keep our bodies on the alkaline side. What most of you probably don’t know is that calcium is alkaline and that our bones serve as a giant buffer system to help keep our bodies alkaline. Every time we eat acid-forming foods a little bit of bone is dissolved so that calcium can be released into the bloodstream to neutralize the acid. (My apologies to any chemists reading this for my gross simplification of a complex biological system).
Consequently, if we want strong bones, we should eat less acid-forming foods and more of alkaline-forming foods. Among acid-forming foods, sodas are the biggest offenders, but meat, eggs, dairy, and grains are all big offenders as well. Alkaline-forming foods include most fruits & vegetables, peas, beans, lentils, seeds and nuts. In simple terms, the typical American diet is designed to dissolve our bones. Calcium from diet or supplementation may be of little use if our diet is destroying our bones as fast as the calcium tries to rebuild them.
#3: Test your blood 25-hydroxyvitamin D level: 25-hydroxy vitamin D is the active form of vitamin D in our bloodstream. We need a sufficient (20-50 ng/mL) blood level of 25-hydroxy vitamin D to be able to use calcium efficiently for bone formation. We now know that some people who seem to be getting adequate vitamin D in their diet still have low 25-hydroxyvitamin D levels. In fact, various studies have shown that somewhere between 20-35% of Americans have insufficient blood levels of 25-hydroxy vitamin D. You should get your blood level tested. If it is low, consult with your health professional on how much vitamin D you need to bring your 25-hydroxy vitamin D into the sufficient range.
#4: Beware of drugs:The list of common medications that dissolve bones is a long one. Some of the worst offenders are anti-inflammatory steroids such as cortisone & prednisone, drugs to treat depression, drugs to treat acid reflux, and excess thyroid hormone.
I’m not suggesting that you avoid prescribed medications that are needed to treat a health condition. I would suggest that you ask your doctor or pharmacist (or research online) whether the drugs you are taking adversely affect bone density. If they do, you may want to ask your doctor about alternative approaches, and you should pay a lot more attention to the other aspects of a “bone healthy” lifestyle.
#5: Exercise is perhaps the most important aspect of a bone healthy lifestyle:Whenever our muscles pull on a bone it stimulates the bone to get stronger. I’ll put the benefits of exercise in perspective in the next section.
Exercise Is A Critical Part of Preventing Osteoporosis
Instead of just quoting more boring studies, I’m going to share a couple of stories that help put the importance of exercise into perspective.
The first is my wife’s story. She ate a very healthy diet with minimal meat and lots of fruits and vegetables for years. She took calcium supplements on a daily basis. She walked 5 miles per day and took yoga classes several days each week. Yet when her doctor recommended a bone density scan in her early sixties she discovered she had low bone density. She was in danger of becoming osteoporotic!
 Her doctor prescribed Fosamax. My wife tried it for one day and decided the side effects were worse than the disease. So she started asking holistic health practitioners what she should do. They recommended she find a personal trainer and start pumping iron. That was not an easy solution, but it was the right one. When she went in for her second bone scan 3 months later, her doctor excitedly announced that her bone density had increased by 7%. Her doctor said “We never get results that good with Fosamax”. When my wife told her she wasn’t taking Fosamax, her doctor became even more excited. (Most doctors actually do prefer holistic approaches. They just don’t recommend them.)
Her doctor prescribed Fosamax. My wife tried it for one day and decided the side effects were worse than the disease. So she started asking holistic health practitioners what she should do. They recommended she find a personal trainer and start pumping iron. That was not an easy solution, but it was the right one. When she went in for her second bone scan 3 months later, her doctor excitedly announced that her bone density had increased by 7%. Her doctor said “We never get results that good with Fosamax”. When my wife told her she wasn’t taking Fosamax, her doctor became even more excited. (Most doctors actually do prefer holistic approaches. They just don’t recommend them.)
The moral of this story is that you can be doing everything else right, but if you’re not doing weight bearing exercises – if you’re not pumping iron, everything else you are doing may be for naught. Weight bearing exercise is an absolutely essential part of a “bone healthy” lifestyle!
But, can exercise do it alone? Some people seem to think so. That brings up my second story. About 30 years ago one of my UNC colleagues, who was an expert on calcium metabolism, was doing a bone density study on female athletes at UNC. One of the tennis players was nicknamed “Tab.” Tab was a popular soft drink at that time, and Tab was all she drank – no milk, no water, only Tab. When my colleague measured the bone density of her playing arm, it was normal for a woman of her age. When he measured the bone density of her non-playing arm, it was that of a 65 year old woman. The reason is simple. When we exercise a particular bone, our body will add calcium to that bone to make it stronger. If we are not getting enough calcium from our diet, our body simply dissolves the bones elsewhere in our body to get the calcium that it needs.
The moral of this story is that exercise alone is not enough. In terms of bone health, we absolutely need exercise to take advantage of the calcium in our diet, and we absolutely need sufficient calcium in our diet to take advantage of the exercise.
This is the most glaring deficiency of the meta-analysis I described last week. None of those studies included exercise. No wonder the increase in bone density was minimal!
Putting It All Together – A “Bone Healthy” Lifestyle
 If you seriously want to minimize your risk of osteoporosis, there are a few simple steps you can take (simple, but not easy).
If you seriously want to minimize your risk of osteoporosis, there are a few simple steps you can take (simple, but not easy).
- Consume a “bone healthy” diet that emphasizes fresh fruits and vegetables, minimizes meats, and eliminates sodas and other acidic beverages. For more details on whether your favorite foods are acid-forming or alkaline-forming, you can find plenty of charts on the internet.
- Minimize the use of medications that adversely affect bone density. You’ll need to work with your doctor on this one.
- Get plenty of weight bearing exercise. This is an absolutely essential part of a bone healthy lifestyle. Your local Y can probably give you guidance if you can’t afford a personal trainer. Of course, if you have physical limitations or have a disease, you should consult with your health professional before beginning any exercise program.
- Get your blood 25-hydroxy vitamin D level tested. If it is low, take enough supplemental vitamin D to get your 25-hydroxy vitamin D level into the sufficient range – optimal is even better. Sufficient blood levels of 25-hydroxy vitamin D are also absolutely essential for you to be able to utilize calcium efficiently.
- Consider a calcium supplement. Even when you are doing everything else correctly, you still need adequate calcium in your diet to form strong bones. “I’m not necessarily recommending a “one-size fits all” 1,000 to 1,200 mg/day. Supplementation is always most effective when you actually need it. For example:
- If you are not including dairy products in your diet (either because they are acid-forming or for other health reasons), it will be difficult for you to get adequate amounts of calcium in your diet. You can get calcium from other food sources such as green leafy vegetables. However, unless you plan your diet very carefully you will probably not get enough.
- If you are taking medications that decrease bone density, that may increase your need for supplemental calcium. Unfortunately, we don’t yet have guidelines on how much is needed.
- If you do use a calcium supplement, make sure it is complete. Don’t just settle for calcium and vitamin D. At the very least you will want your supplement to contain magnesium and vitamin K. I personally recommend that it also contain zinc, copper, and manganese.
- Unfortunately, we don’t really have good guidelines for how much calcium you need. Studies like the one described above are challenging the old RDAs, but we don’t yet have enough studies to know how much calcium we need to build strong bones when we are following a “bone healthy” lifestyle that includes proper diet, sufficient 25-hydroxy vitamin D blood levels and plenty of exercise.
What About Medications For Preventing Bone Loss?
The danger is that, as the conclusions of this meta-analysis get widely publicized and doctors stop prescribing calcium supplements, they probably aren’t going to recommend a holistic approach. They probably won’t recommend a “bone healthy” lifestyle. Instead, they will most  likely recommend drugs to prevent bone loss. In fact, the authors of the study described last week specifically praised the use of bisphosphonate drugs (Fosamax and Zometa), and a related drug (Xgeva) that works by a similar mechanism because they increased bone density by 5-9% over 3 years.
likely recommend drugs to prevent bone loss. In fact, the authors of the study described last week specifically praised the use of bisphosphonate drugs (Fosamax and Zometa), and a related drug (Xgeva) that works by a similar mechanism because they increased bone density by 5-9% over 3 years.
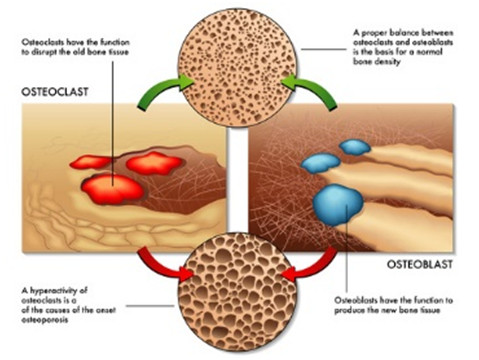
However, these drugs have a dark side, and it’s not just the acid reflux, esophageal damage and esophageal cancer that you hear about in the TV ads. These drugs all act by blocking bone resorption, the ability of the body to break down bone. In the short term, this prevents the bone loss associated with aging and reduces the risk of bone fractures.
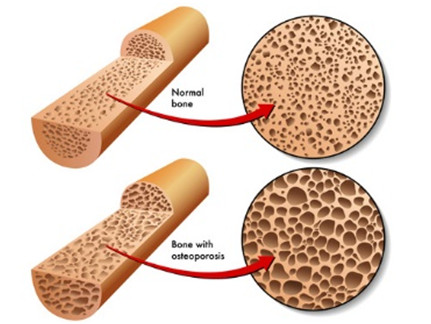
However, you might remember from last week’s article that bone resorption is also an essential part of bone remodeling, the process that keeps our bones young and strong. When these drugs are used for more than a few years you end up with bones that are dense, but are also old and brittle. Long term use of these drugs is associated with jaw bones that simply dissolve and bones that easily break during everyday activities. This is yet another example of drugs with side effects that look a lot like the disease you were taking the drug for in the first place.
The Bottom Line
- A recent study has reported that the RDA recommendation of 1,000 – 1,200 mg/day of calcium for people over 50 provides only a minimal increase in bone density (0.7-1.8%) over the first year or two. This translates into a very small (5-10%) decrease in risk of bone fractures. It did not matter whether the calcium came from dietary sources or from supplementation. The authors concluded that adding extra calcium to the diet, whether from foods or supplements, was not a very efficient way to increase bone density and prevent fractures.
2. This study suffers from some serious flaws, which I discussed in last week’s “Health Tips From the Professor”
3. Unfortunately, many doctors are likely to take this study to heart. They are likely to stop recommending calcium and other natural approaches and start relying even more heavily on drugs to preserve bone mass. That’s bad news because, while the most frequently proscribed drugs do increase bone mass and prevent fractures short term, they also cause your bones to age more rapidly. After a few years you end up with bones that are dense, but are also incredibly brittle and fracture very easily. That’s right. If you use these drugs long enough, they will cause the very condition you were trying to prevent.
4. We should also consider the possibility that this study may just be correct. Let’s assume for a minute that the RDA recommendation of 1,000 – 1,200 mg/day of calcium for everyone over 50 may actually be flawed advice. If so, it may finally be time to put away the “magic bullet” thinking and start seriously considering holistic approaches to preserving bone mass.
5. A far better choice is to follow a “bone healthy” lifestyle.
- Start with a “bone healthy” diet. Avoid acid-forming foods like sodas, meats, eggs, dairy, and grains. Instead choose alkaline-forming foods like most fruits & vegetables, peas, beans, lentils, seeds and nuts.
- Check on the medicines you are using. If they are ones that adversely affect bone density, ask your health professional if there are bone-healthier options.
- Check your blood level of 25-hydroxy vitamin D on a regular basis. If it is low, consult with your health professional on the amount of vitamin D you need to take to bring your 25-hydroxy vitamin D into the optimal range.
- Get plenty of weight bearing exercise. This means pumping iron. It is an absolutely essential part of a bone healthy lifestyle. Of course, if you have physical limitations or have a disease, you should consult with your health professional before beginning any exercise program.
- If you are not getting sufficient calcium from your diet, consider a complete calcium supplement. In addition to calcium and vitamin D, a bone-healthy calcium supplement should at the very least contain magnesium and vitamin K. I also recommend it contain zinc, copper, and manganese.
Just don’t rely on a calcium supplement alone to keep your bone density where it should be. If your 25-hydroxy vitamin D isn’t where it should be and/or you aren’t doing weight bearing exercise on a regular basis, your calcium supplement may be almost useless. All the aforementioned may aid in preventing osteoporosis. In my opinion, that may be the biggest take-home lesson from the recent meta-analysis.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure or prevent any disease.
 Usually I review scholarly publications of clinical studies, but occasionally I find an article in the popular press that’s so good I just have to share it with you. The lead article about weight loss by Bonnie Liebman in the April 2015 issue of Nutrition Action is just such an article. She called it “8 Weight Mistakes”, but I think “8 Weight Loss Myths” would be a better title.
Usually I review scholarly publications of clinical studies, but occasionally I find an article in the popular press that’s so good I just have to share it with you. The lead article about weight loss by Bonnie Liebman in the April 2015 issue of Nutrition Action is just such an article. She called it “8 Weight Mistakes”, but I think “8 Weight Loss Myths” would be a better title. On most diets you lose muscle as well as fat. I have talked about this in a previous article, High Protein Diets and Weight Loss , but muscle is important because it burns off calories much faster than fat.
On most diets you lose muscle as well as fat. I have talked about this in a previous article, High Protein Diets and Weight Loss , but muscle is important because it burns off calories much faster than fat.
 You’ve heard this one before. However, even on the most successful diets, weight loss is temporary. Most people eventually regain all the weight they’ve lost and more. Again I’ve also covered the reason for this in my “3 Things Every Successful Diet Must Do” eBook, which is available at Health Tips From the Professor. To spare you the trouble of reading the book I will share the secret with you. Simply put: “Diets never work long term. Only true lifestyle change can lead to long term weight loss.”
You’ve heard this one before. However, even on the most successful diets, weight loss is temporary. Most people eventually regain all the weight they’ve lost and more. Again I’ve also covered the reason for this in my “3 Things Every Successful Diet Must Do” eBook, which is available at Health Tips From the Professor. To spare you the trouble of reading the book I will share the secret with you. Simply put: “Diets never work long term. Only true lifestyle change can lead to long term weight loss.” (2.6 billion new fat cells for every 3.5 pounds of fat). Once you add that extra fat to your lower body you’re pretty much stuck with it.
(2.6 billion new fat cells for every 3.5 pounds of fat). Once you add that extra fat to your lower body you’re pretty much stuck with it. Many Americans cling to the false hope that they can eat whatever they want as long as they take some sort of magic herb or pill to boost their metabolism. The fact is that natural metabolic boosters like green tea have a very modest effect on metabolism. They can play a role in a well-designed diet program, but they will never allow you to eat whatever you want and lose weight.
Many Americans cling to the false hope that they can eat whatever they want as long as they take some sort of magic herb or pill to boost their metabolism. The fact is that natural metabolic boosters like green tea have a very modest effect on metabolism. They can play a role in a well-designed diet program, but they will never allow you to eat whatever you want and lose weight. This is perhaps the most pervasive myth of all. This is the one that sells millions of gym memberships every January.
This is perhaps the most pervasive myth of all. This is the one that sells millions of gym memberships every January.