Can ADHD Be Prevented?
 If you are pregnant, or of childbearing age, should you be supplementing with vitamin D? Increasingly, the answer appears to be yes.
If you are pregnant, or of childbearing age, should you be supplementing with vitamin D? Increasingly, the answer appears to be yes.
1) Based on blood 25-hydroxy vitamin D levels (considered the most accurate marker of vitamin D status):
-
- 8-11% of pregnant women in the US are deficient in vitamin D (<30 nmol/L).
-
- 25% of pregnant women have insufficient vitamin D status (30-49 nmol/L).
In short, that means around 1/3 of pregnant women in the US have insufficient or deficient levels of vitamin D. The effect of inadequate vitamin D during pregnancy is not just an academic question.
2) The Cochrane Collaboration (considered the gold standard for evidence-based medicine) has recently concluded that supplementation with vitamin D reduces the risk of significant complications during pregnancy.
3) Another recent study found that inadequate vitamin D status during pregnancy delayed several neurodevelopmental milestones in early childhood, including gross motor skills, fine motor skills, and social development.
If neurodevelopmental milestones are affected, what about ADHD? Here the evidence is not as clear. Some studies have concluded that vitamin D deficiency during pregnancy increases the risk of ADHD in the offspring. Other studies have concluded there is no effect of vitamin D deficiency on ADHD.
Why the discrepancy between studies?
- Most of the previous studies have been small. Simply put, there were too few children in the study to make statistically reliable conclusions.
- Most of the studies measured maternal 25-hydroxyvitamin D levels in the third trimester or in chord blood at birth. However, it is during early pregnancy that critical steps in the development of the nervous system take place.
Thus, there is a critical need for larger studies that measure maternal vitamin D status in the first trimester of pregnancy. This study (M Sucksdorff et al, Journal of the American Academy of Child & Adolescent Psychiatry, 2020, in press) was designed to fill that need.
How Was The Study Done?
 This study compared 1,067 Finnish children born between 1998 and 1999 who were subsequently diagnosed with ADHD and 1,067 matched controls without ADHD. There were several reasons for choosing this experimental group.
This study compared 1,067 Finnish children born between 1998 and 1999 who were subsequently diagnosed with ADHD and 1,067 matched controls without ADHD. There were several reasons for choosing this experimental group.
- Finland is among the northernmost European countries, so sun exposure during the winter is significantly less than for the United States and most other European countries. This time period also preceded the universal supplementation with vitamin D for pregnant women that was instituted in 2004.
Consequently, maternal 25-hydroxyvitamin D levels were significantly lower than in most other countries. This means that a significant percentage of pregnant women were deficient in vitamin D, something not seen in most other studies. For example:
-
- 49% of pregnant women in Finland were deficient in vitamin D (25-hydoxyvitamin D <30 nmol/L) compared to 8-11% in the United States.
-
- 33% of pregnant women in Finland had insufficient vitamin D status (25-hydroxyvitamin D 30-49.9 nmol/L) compared to 25% in the United States.
- Finland, like many European countries, keeps detailed health records on its citizens. For example:
-
- The Finnish Prenatal Study collected data, including maternal 25-hydroxyvitamin D levels during the first trimester), for all live births between 1991 and 2005.
-
- The Care Register for Health Care recorded, among other things, all diagnoses of ADHD through 2011.
Thus, this study was ideally positioned to compare maternal 25-hydroxyvitamin D levels during the first trimester of pregnancy with a subsequent diagnosis of ADHD in the offspring. The long-term follow-up was important to this study because the average age of ADHD diagnosis was 7 years (range = 2-14 years).
Does Maternal Vitamin D Affect Childhood ADHD?
 The answer to this question appears to be a clear, yes.
The answer to this question appears to be a clear, yes.
If you divide maternal vitamin D levels into quintiles:
- Offspring of mothers in the lowest vitamin D quintile (25-hydroxyvitamin D of 7.5-21.9 nmol/L) were 53% more likely to develop ADHD than offspring of mothers in the highest vitamin D quintile (49.5-132.5 nmol/L).
When you divide maternal vitamin D levels by the standard designations of deficient (<30 nmol/L), insufficient (30-49.9 nmol/L), and sufficient (≥50 nmol/L):
- Offspring of mothers who were deficient in vitamin D were 34% more likely to develop ADHD than children of mothers with sufficient vitamin D status.
The authors concluded: “This is the first population-based study to demonstrate an association between low maternal vitamin D during the first trimester of pregnancy and an elevated risk for ADHD diagnosis in offspring. If these findings are replicated, they may have public health implications for vitamin D supplementation and perhaps changing lifestyle behaviors during pregnancy to ensure optimal maternal vitamin D levels.”
Can ADHD Be Prevented?
 I realize that this is an emotionally charged title. If you have a child with ADHD, the last thing I want is for you to feel guilty about something you may not have done. So, let me start by acknowledging that there are genetic and environmental risk factors for ADHD that you cannot control. That means you could have done everything right during pregnancy and still have a child who develops ADHD.
I realize that this is an emotionally charged title. If you have a child with ADHD, the last thing I want is for you to feel guilty about something you may not have done. So, let me start by acknowledging that there are genetic and environmental risk factors for ADHD that you cannot control. That means you could have done everything right during pregnancy and still have a child who develops ADHD.
Having said that, let’s examine things that can be done to reduce the risk of giving birth to a child who will develop ADHD, starting with vitamin D. There are two aspects of this study that are important to keep in mind.
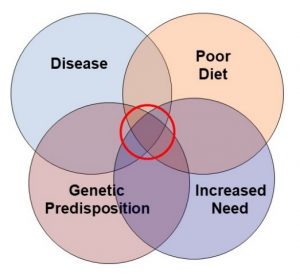
#1: The increased risk of giving birth to a child who develops ADHD was only seen for women who were vitamin D deficient. While vitamin D deficiency is only found in 8-11% of pregnant mothers in the United States, that is an average number. It is more useful to ask who is most likely to be vitamin D deficient in this country. For example:
- Fatty fish and vitamin D-fortified dairy products are the most important food sources of vitamin D. Fatty fish are not everyone’s favorite and may be too expensive for those on a tight budget. Many people are lactose intolerant or avoid milk for other reasons. If you are not eating these foods, you may not be getting enough vitamin D from your diet. This is particularly true for vegans.
- If you have darker colored skin, you may have trouble making enough vitamin D from sunlight. If you are also lactose intolerant, you are in double trouble with respect to vitamin D sufficiency.
- Obesity affects the distribution of vitamin D in the body. So, if you are overweight, you may have low 25-hydroxyvitamin D levels in your blood.
- The vitamin D RDA for pregnant and lactating women is 600 IU, but many multivitamin and prenatal supplements only provide 400 IU. If you are pregnant or of childbearing age, it is a good idea to look for a multivitamin or prenatal supplement that provides at least 600 IU, especially if you are in one of the high risk groups listed above.
- Some experts recommend 2,000 to 4,000 IU of supplemental vitamin D. I would not recommend exceeding that amount without discussing it with your health care provider first.
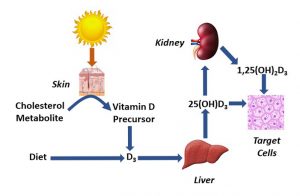
- Finally, for reasons we do not understand, some people have a difficult time converting vitamin D to the active 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D in their bodies. If you are pregnant or of childbearing age, it is a good idea to have your blood 25-hydroxyvitamin D levels determined and discuss with your health care provider how much vitamin D you should be taking. Many people need more than 600 IU to reach vitamin D sufficiency status.
#2: Maternal vitamin D deficiency has a relatively small effect (34%) on the risk of the offspring developing ADHD. That means assuring adequate vitamin D status during pregnancy should be part of a holistic approach for reducing ADHD risk. Other factors to consider are:
- Low maternal folate and omega-3 status.
- Smoking, drug, and alcohol use.
- Obesity.
- Sodas and highly processed foods.
Alone, each of these factors has a small and uncertain influence on the risk of your child developing ADHD. Together, they may play a significant role in determining your child’s risk of developing ADHD.
In closing, there are three take-home lessons I want to leave you with:
1) The first is that there is no “magic bullet”. There is no single action you can take during pregnancy that will dramatically reduce your risk of giving birth to a child who will develop ADHD. Improving your vitamin D, folate, and omega-3 status; avoiding cigarettes, drugs, and alcohol; achieving a healthy weight; and eating a healthy diet are all part of a holistic approach for reducing the risk of your child developing ADHD.
2) The second is that we should not think of these actions solely in terms of reducing ADHD risk. Each of these actions will lead to a healthier pregnancy and a healthier child in many other ways.
3) Finally, if you have a child with ADHD and would like to reduce the symptoms without drugs, I recommend this article.
The Bottom Line
A recent study looked at the correlation between maternal vitamin D status during the first trimester of pregnancy and the risk of ADHD in the offspring. The study found:
- Offspring of mothers who were deficient in vitamin D were 34% more likely to develop ADHD than children of mothers with sufficient vitamin D status.
The authors concluded: “This is the first population-based study to demonstrate an association between low maternal vitamin D during the first trimester of pregnancy and an elevated risk for ADHD diagnosis in offspring. If these findings are replicated, they may have public health implications for vitamin D supplementation and perhaps changing lifestyle behaviors during pregnancy to ensure optimal maternal vitamin D levels.”
In the article above I discuss what this study means for you and other factors that increase the risk of giving birth to a child who will develop ADHD.
For more details read the article above.
These statements have not been evaluated by the Food and Drug Administration. This information is not intended to diagnose, treat, cure, or prevent any disease.